

Early-childhood linear growth faltering in low- and middle-income countries
- PMID: 37704719
- PMCID: PMC10511325
- DOI: 10.1038/s41586-023-06418-5
Early-childhood linear growth faltering in low- and middle-income countries
Erratum in
-
Author Correction: Early-childhood linear growth faltering in low- and middle-income countries.Nature. 2023 Nov;623(7985):E2. doi: 10.1038/s41586-023-06703-3. Nature. 2023. PMID: 37833392 Free PMC article. No abstract available.
-
Author Correction: Early-childhood linear growth faltering in low- and middle-income countries.Nature. 2025 Jan;637(8045):E18. doi: 10.1038/s41586-024-08344-6. Nature. 2025. PMID: 39668242 Free PMC article. No abstract available.
Abstract
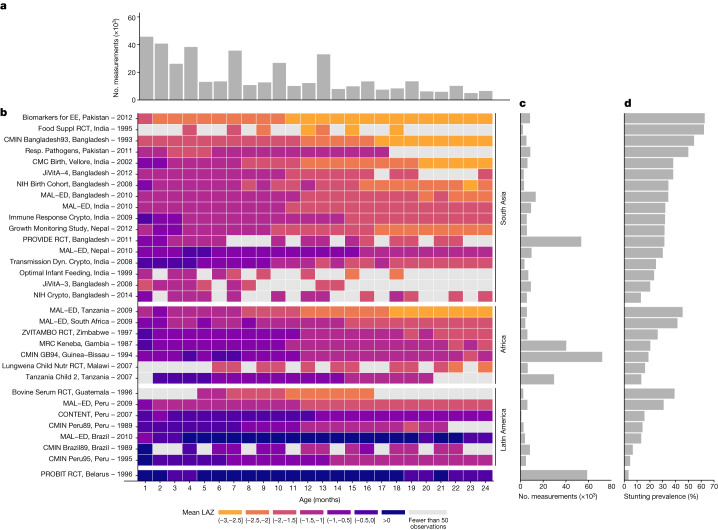
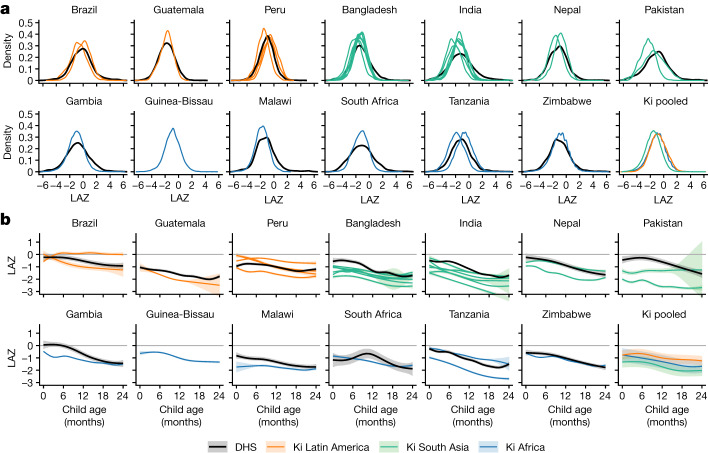
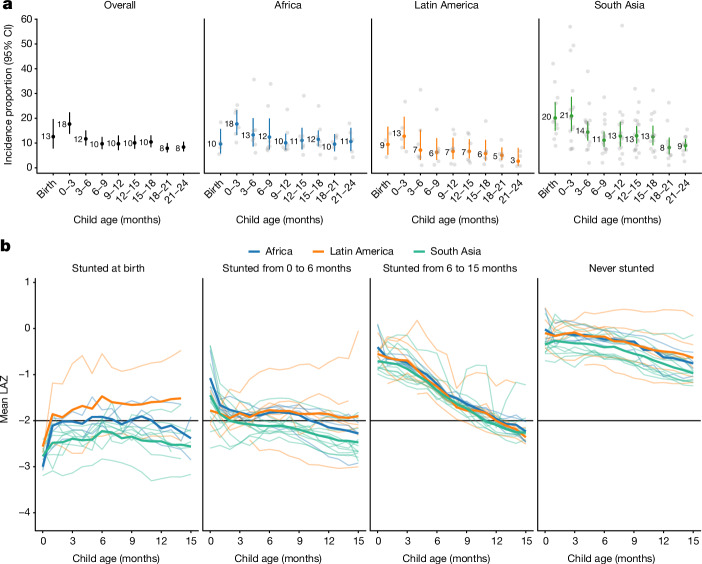
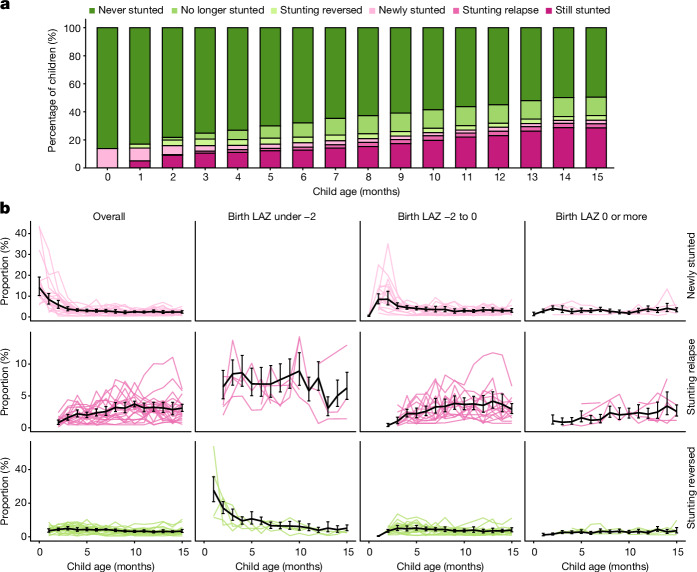
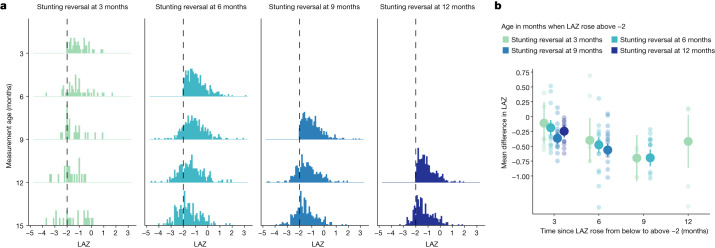
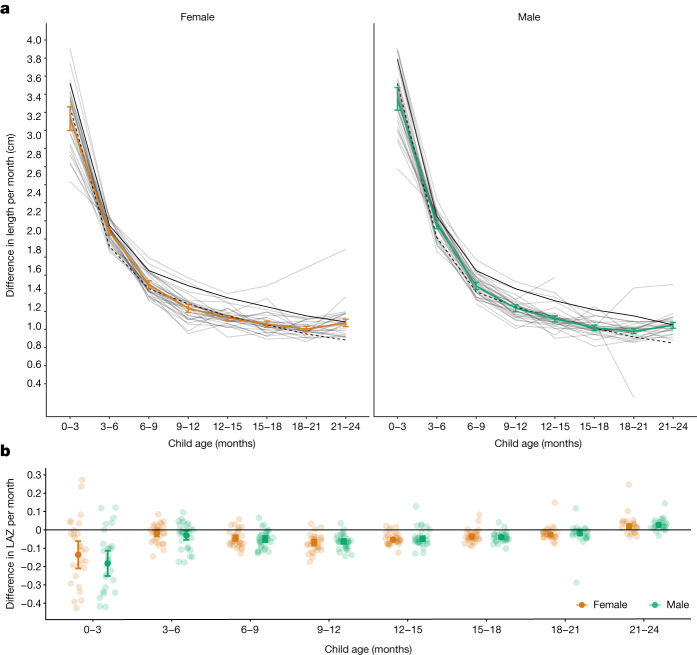
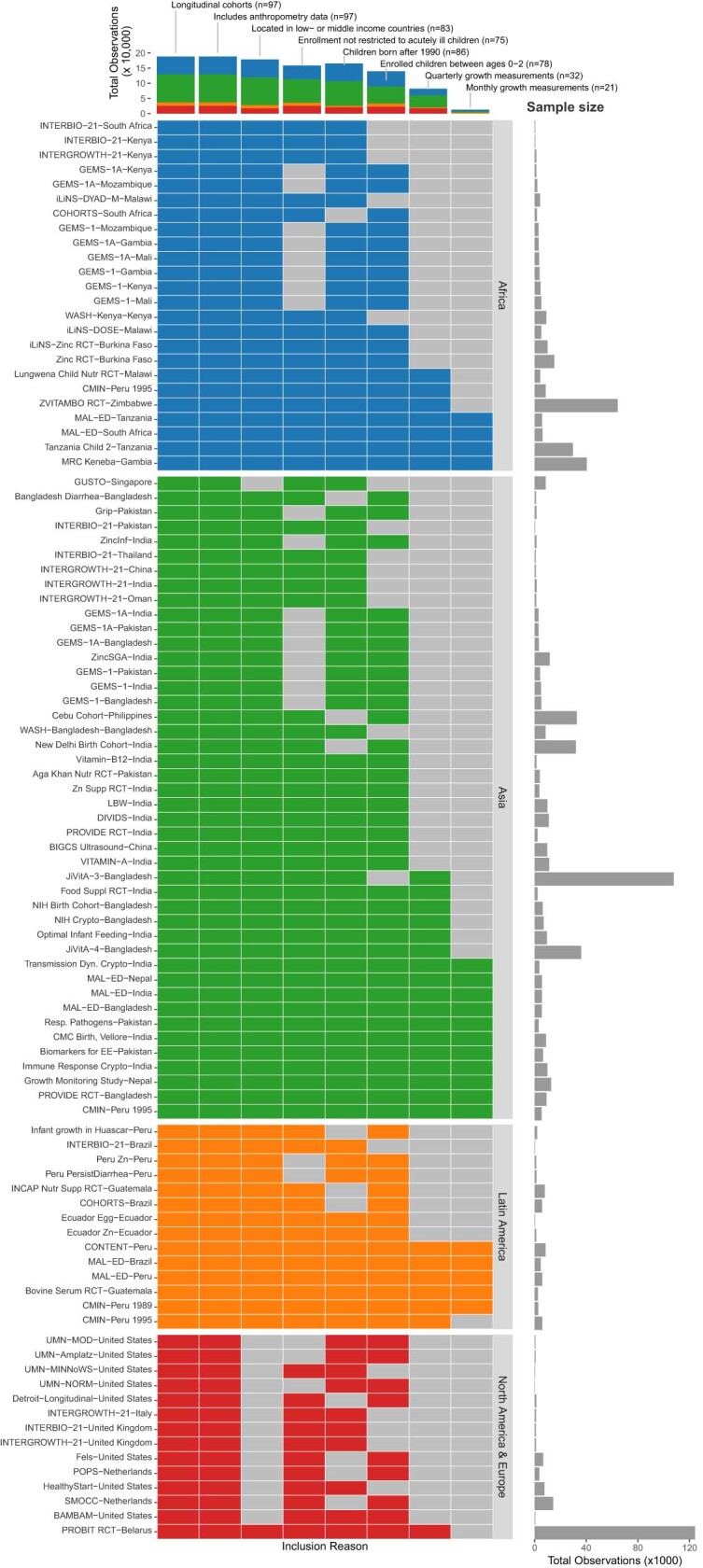
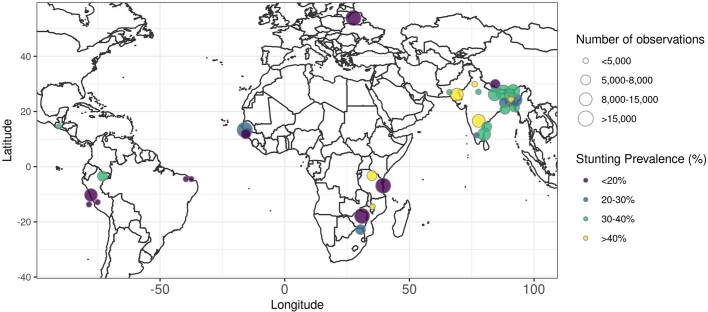
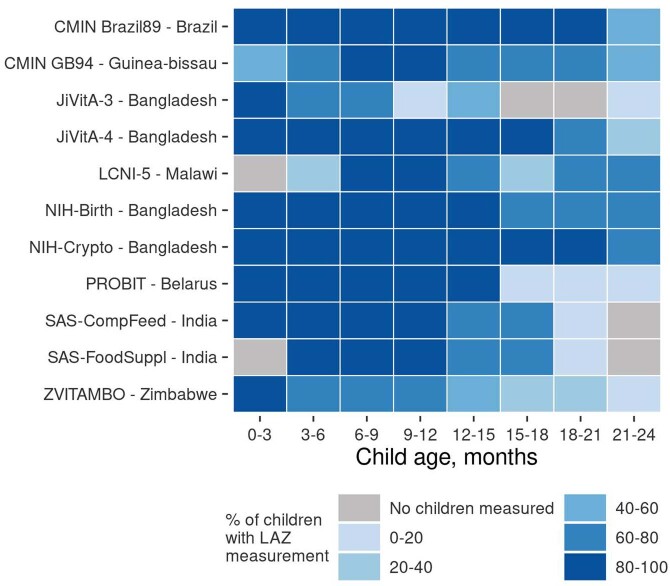
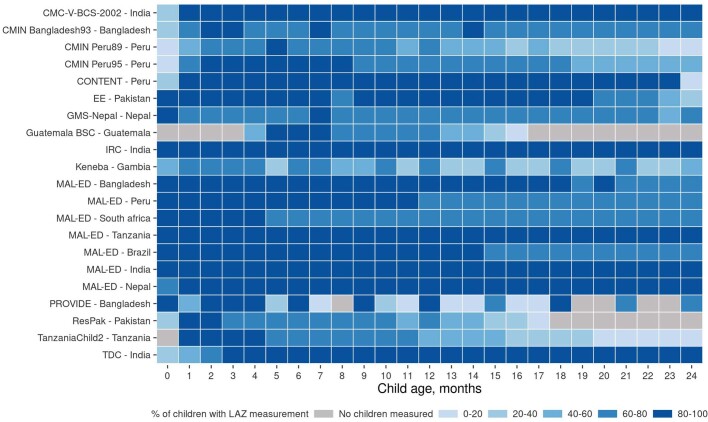
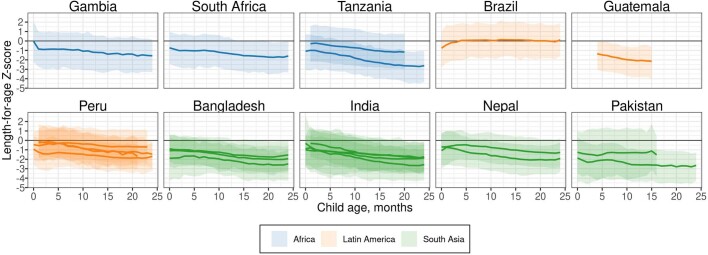
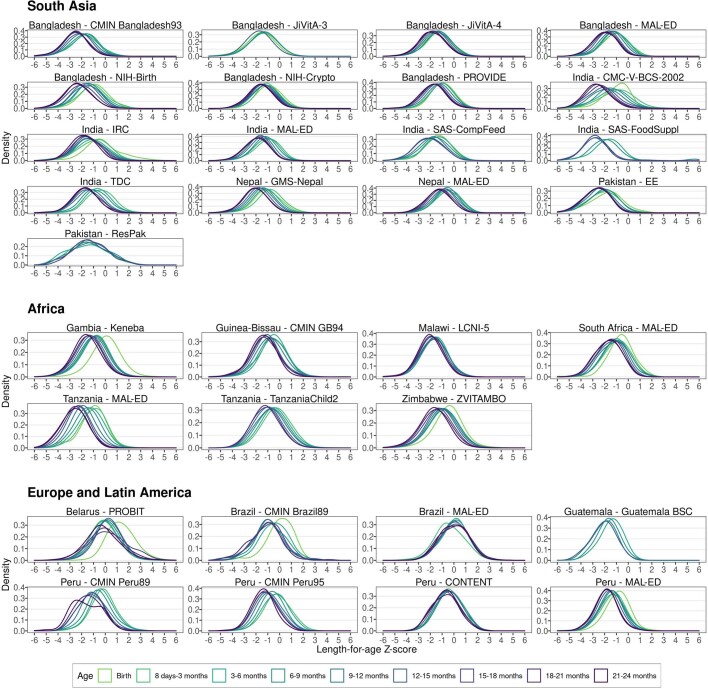
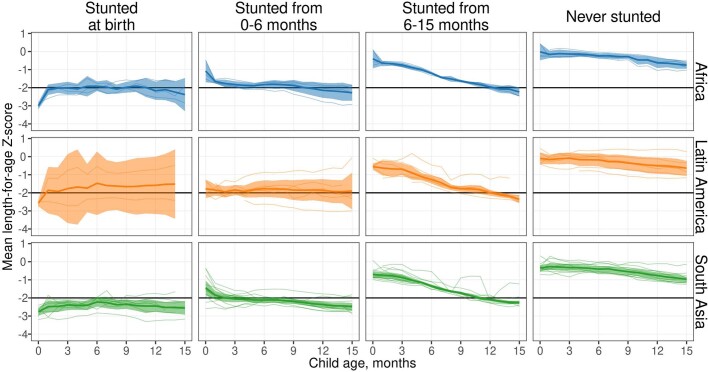
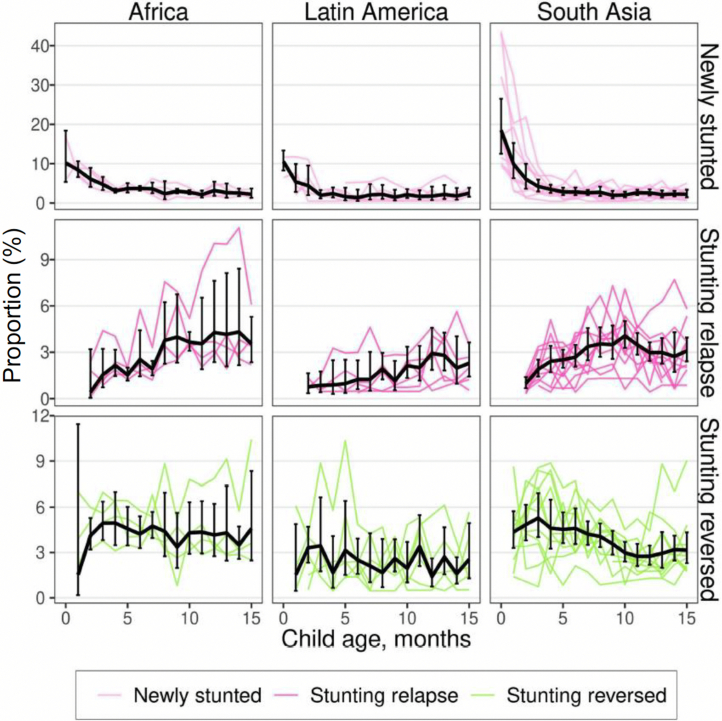
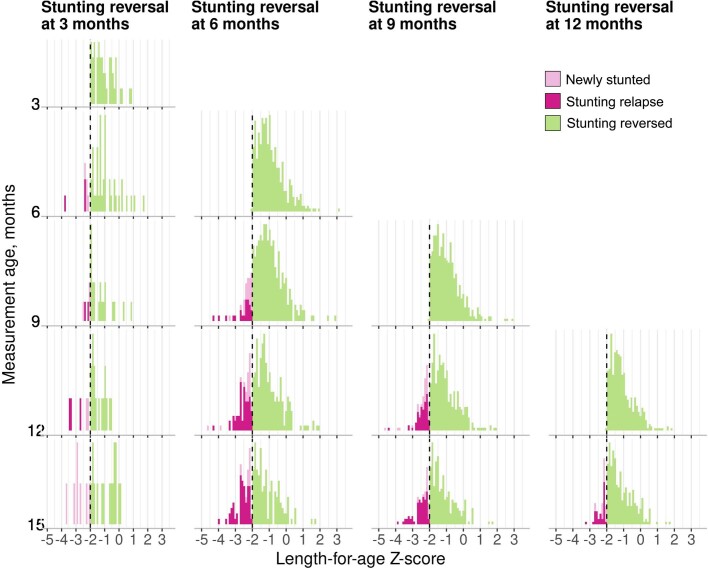
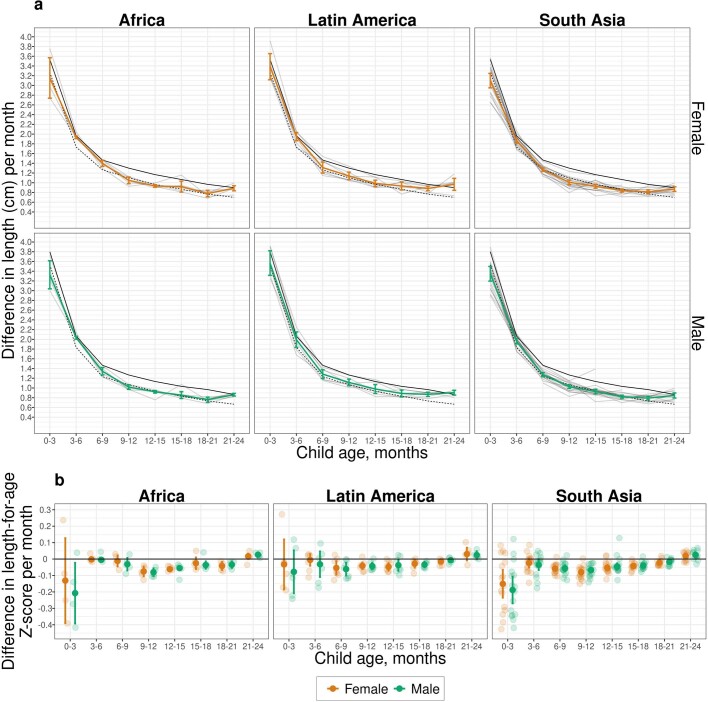
Globally, 149 million children under 5 years of age are estimated to be stunted (length more than 2 standard deviations below international growth standards)1,2. Stunting, a form of linear growth faltering, increases the risk of illness, impaired cognitive development and mortality. Global stunting estimates rely on cross-sectional surveys, which cannot provide direct information about the timing of onset or persistence of growth faltering-a key consideration for defining critical windows to deliver preventive interventions. Here we completed a pooled analysis of longitudinal studies in low- and middle-income countries (n = 32 cohorts, 52,640 children, ages 0-24 months), allowing us to identify the typical age of onset of linear growth faltering and to investigate recurrent faltering in early life. The highest incidence of stunting onset occurred from birth to the age of 3 months, with substantially higher stunting at birth in South Asia. From 0 to 15 months, stunting reversal was rare; children who reversed their stunting status frequently relapsed, and relapse rates were substantially higher among children born stunted. Early onset and low reversal rates suggest that improving children's linear growth will require life course interventions for women of childbearing age and a greater emphasis on interventions for children under 6 months of age.
© 2023. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
T.N. is an employee of the Bill & Melinda Gates Foundation. P.C. is a former employee of the Bill & Melinda Gates Foundation, and K.H.B. is a former employee of and occasional consultant to the Bill & Melinda Gates Foundation. J.C., V.S., R. Hafen and J.H. work as research contractors financially supported by the Bill & Melinda Gates Foundation.
Figures
References
-
- Levels and Trends in Child Malnutrition: Key Findings of the 2019 Editionof the Joint Child Malnutrition Estimates (UNICEF, WHO & World Bank, 2019); https://www.unicef.org/media/60626/file/Joint-malnutrition-estimates-201....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
