

Assessing and Understanding Reactance, Self-Exemption, Disbelief, Source Derogation and Information Conflict in Reaction to Overdiagnosis in Mammography Screening: Scale Development and Preliminary Validation
- PMID: 37705500
- PMCID: PMC10843591
- DOI: 10.1177/0272989X231195603
Assessing and Understanding Reactance, Self-Exemption, Disbelief, Source Derogation and Information Conflict in Reaction to Overdiagnosis in Mammography Screening: Scale Development and Preliminary Validation
Abstract
Purpose: Overdiagnosis is a concept central to making informed breast cancer screening decisions, and yet some people may react to overdiagnosis with doubt and skepticism. The present research assessed 4 related reactions to overdiagnosis: reactance, self-exemption, disbelief, and source derogation (REDS). The degree to which the concept of overdiagnosis conflicts with participants' prior beliefs and health messages (information conflict) was also assessed as a potential antecedent of REDS. We developed a scale to assess these reactions, evaluated how those reactions are related, and identified their potential implications for screening decision making.
Methods: Female participants aged 39 to 49 years read information about overdiagnosis in mammography screening and completed survey questions assessing their reactions to that information. We used a multidimensional theoretical framework to assess dimensionality and overall domain-specific internal consistency of the REDS and Information Conflict questions. Exploratory and confirmatory factor analyses were performed using data randomly split into a training set and test set. Correlations between REDS, screening intentions, and other outcomes were evaluated.
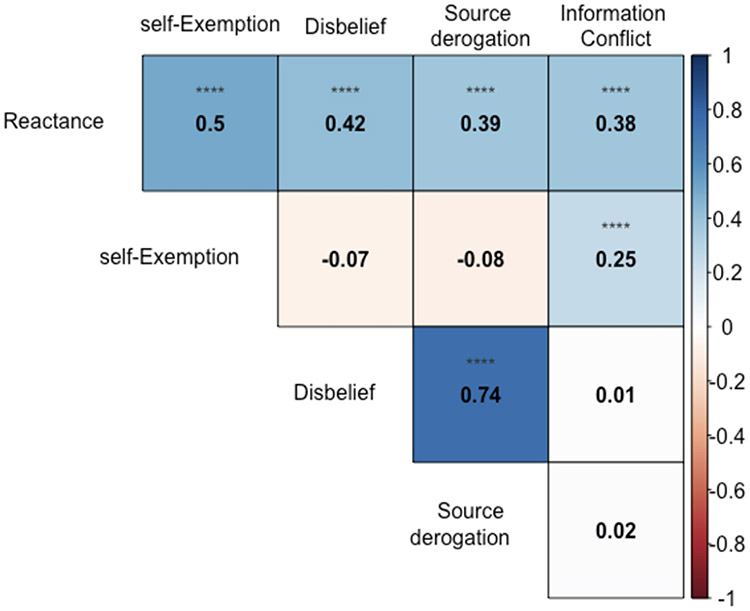
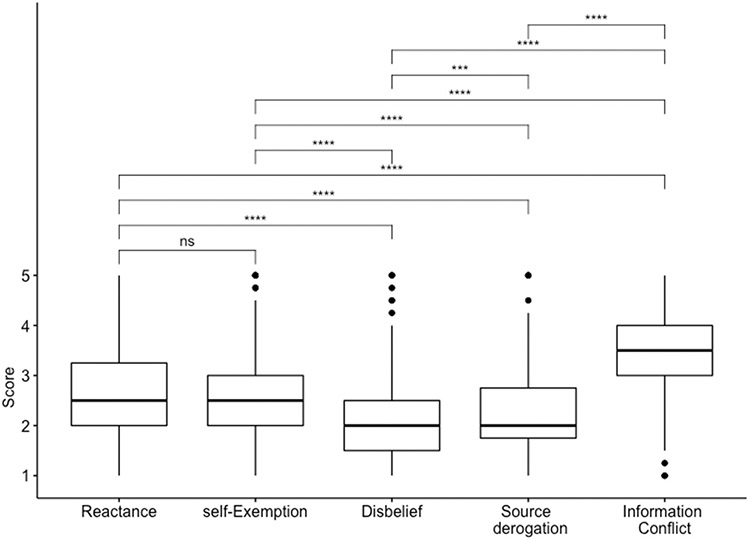
Results: Five-hundred twenty-five participants completed an online survey. Exploratory and confirmatory factor analyses identified that Reactance, Self Exemption, Disbelief, Source Derogation, and Information Conflict represent unique constructs. A reduced 20-item scale was created by selecting 4 items per construct, which showed good model fit. Reactance, Disbelief, and Source Derogation were associated with lower intent to use information about overdiagnosis in decision making and the belief that informing people about overdiagnosis is unimportant.
Conclusions: REDS and Information Conflict are distinct but correlated constructs that are common reactions to overdiagnosis. Some of these reactions may have negative implications for making informed screening decisions.
Highlights: Overdiagnosis is a concept central to making informed breast cancer screening decisions, and yet when provided information about overdiagnosis, some people are skeptical.This research developed a measure that assessed different ways in which people might express skepticism about overdiagnosis (reactance, self-exemption, disbelief, source derogation) and also the perception that overdiagnosis conflicts with prior knowledge and health messages (information conflict).These different reactions are distinct but correlated and are common reactions when people learn about overdiagnosis.Reactance, disbelief, and source derogation are associated with lower intent to use information about overdiagnosis in decision making as well as the belief that informing people about overdiagnosis is unimportant.
Keywords: breast cancer screening; decision-making; disbelief; overdiagnosis; skepticism.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant from the National Cancer Institute, R37CA254926. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Figures
References
-
- Berkman ND, Sheridan SL, Donahue KE, et al. The Effect of Interventions To Mitigate the Effects of Low Health Literacy. Published March 2011. Accessed January 27, 2014. http://www.ncbi.nlm.nih.gov/books/NBK82433/
-
- DeWalt DA, Pignone MP. Reading is fundamental: the relationship between literacy and health. Archives of internal medicine. 2005;165(17):1943. - PubMed
-
- Fagerlin A, Ubel PA, Smith DM, Zikmund-Fisher BJ. Making numbers matter: present and future research in risk communication. American Journal of Health Behavior. 2007;31(Supplement 1):S47–S56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
