

Evaluation of the clinical feasibility of cone-beam computed tomography guided online adaption for simulation-free palliative radiotherapy
- PMID: 37705690
- PMCID: PMC10495619
- DOI: 10.1016/j.phro.2023.100490
Evaluation of the clinical feasibility of cone-beam computed tomography guided online adaption for simulation-free palliative radiotherapy
Abstract
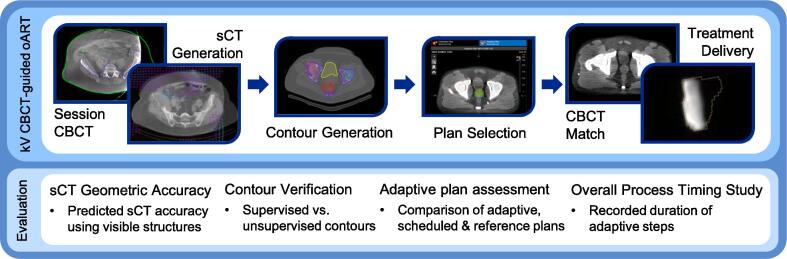
Background and purpose: Simulation-free radiotherapy, where diagnostic imaging is used for treatment planning, improves accessibility of radiotherapy for eligible palliative patients. Combining this pathway with online adaptive radiotherapy (oART) may improve accuracy of treatment, expanding the number of eligible patients. This study evaluated the adaptive process duration, plan dose volume histogram (DVH) metrics and geometric accuracy of a commercial cone-beam computed tomography (CBCT)-guided oART system for simulation-free, palliative radiotherapy.
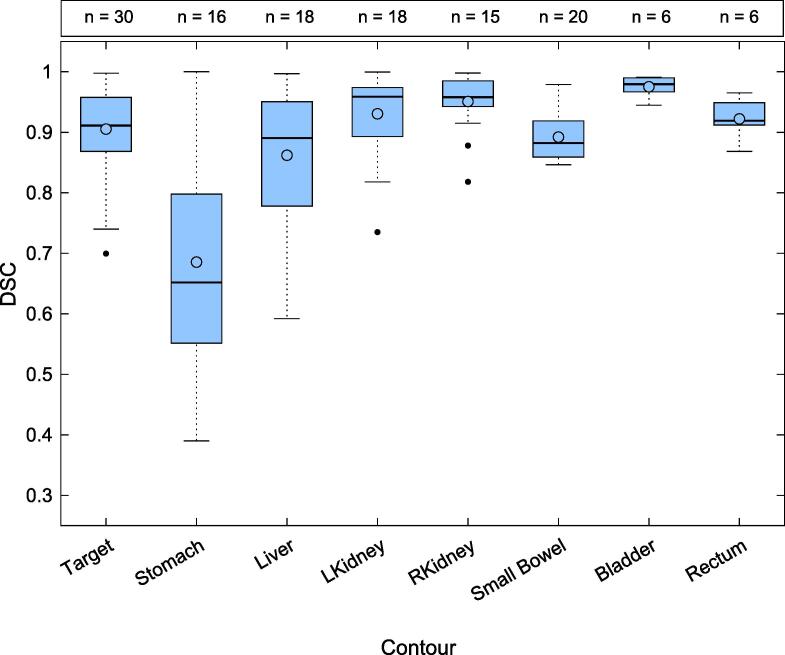
Materials and methods: Ten previously treated palliative cases were used to compare system-generated contours against clinician contours in a test environment with Dice Similarity Coefficient (DSC). Twenty simulation-free palliative patients were treated clinically using CBCT-guided oART. Analysis of oART clinical treatment data included; evaluation of the geometric accuracy of system-generated synthetic CT relative to session CBCT anatomy using a Likert scale, comparison of adaptive plan dose distributions to unadapted, using DVH metrics and recording the duration of key steps in the oART workflow.
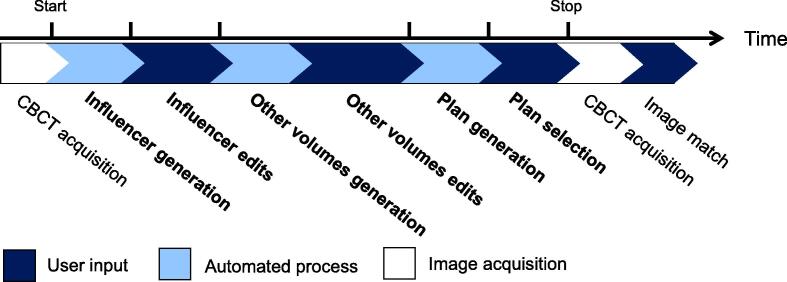
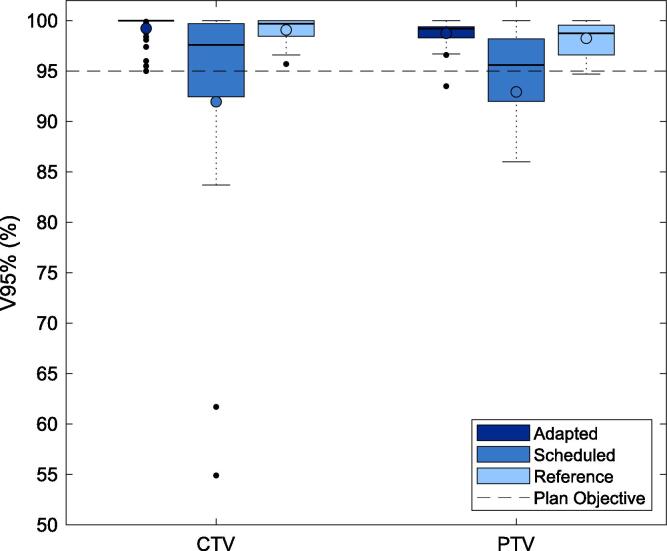
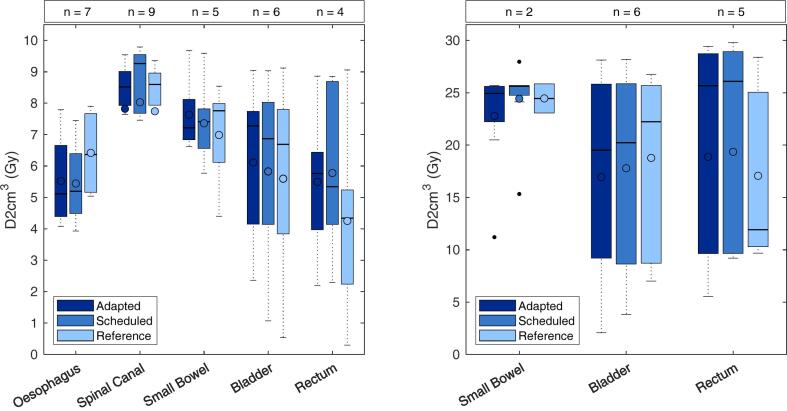
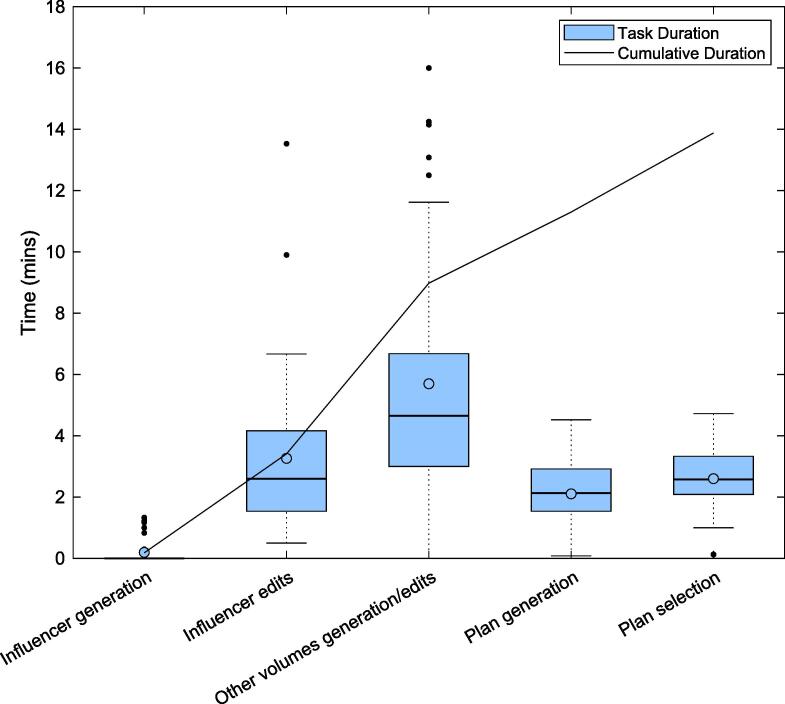
Results: Auto-generated contours achieved a DSC of higher than 0.85, excluding the stomach which was attributed to CBCT image quality issues. Synthetic CT was locally aligned to CBCT anatomy for approximately 80% of fractions, with the remaining suboptimal yet clinically acceptable. Adaptive plans achieved a median CTV V95% of 99.5%, compared to 95.6% for unadapted. The median overall oART process duration was found to be 13.2 mins, with contour editing being the most time-intensive adaptive step.
Conclusions: The CBCT-guided oART system utilising a simulation-free planning approach was found to be sufficiently accurate for clinical implementation, this may further streamline and improve care for palliative patients.
Keywords: Online adaption; Palliative; Radiotherapy; Simulation-free radiotherapy.
© 2023 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Collaborative research agreement with Varian Medical Systems that partially funded this study.
Figures
References
-
- International Atomic Energy Agency, 2012, Radiotherapy in Palliative Cancer Care: Development and Implementation, IAEA Human Health Reports No. 2, IAEA, Vienna.
-
- Wong R.K., Letourneau D., Varma A., Bissonnette J.P., Fitzpatrick D., Grabarz D., et al. A one-step cone-beam CT-enabled planning-to-treatment model for palliative radiotherapy-from development to implementation. Int J Radiat Oncol Biol Phys. 2012;84:834–840. doi: 10.1016/j.ijrobp.2012.01.025. - DOI - PubMed
-
- Held M., Cremers F., Sneed P.K., Braunstein S., Fogh S.E., Nakamura J., et al. Assessment of image quality and dose calculation accuracy on kV CBCT, MV CBCT, and MV CT images for urgent palliative radiotherapy treatments. J Appl Clin Med Phys. 2016;17:279–290. doi: 10.1120/jacmp.v17i2.6040. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
