

Discriminative performance of pancreatic stone protein in predicting ICU mortality and infection severity in adult patients with infection: a systematic review and individual patient level meta-analysis
- PMID: 37707744
- PMCID: PMC10665254
- DOI: 10.1007/s15010-023-02093-w
Discriminative performance of pancreatic stone protein in predicting ICU mortality and infection severity in adult patients with infection: a systematic review and individual patient level meta-analysis
Abstract
Background: Several studies suggested pancreatic stone protein (PSP) as a promising biomarker to predict mortality among patients with severe infection. The objective of the study was to evaluate the performance of PSP in predicting intensive care unit (ICU) mortality and infection severity among critically ill adults admitted to the hospital for infection.
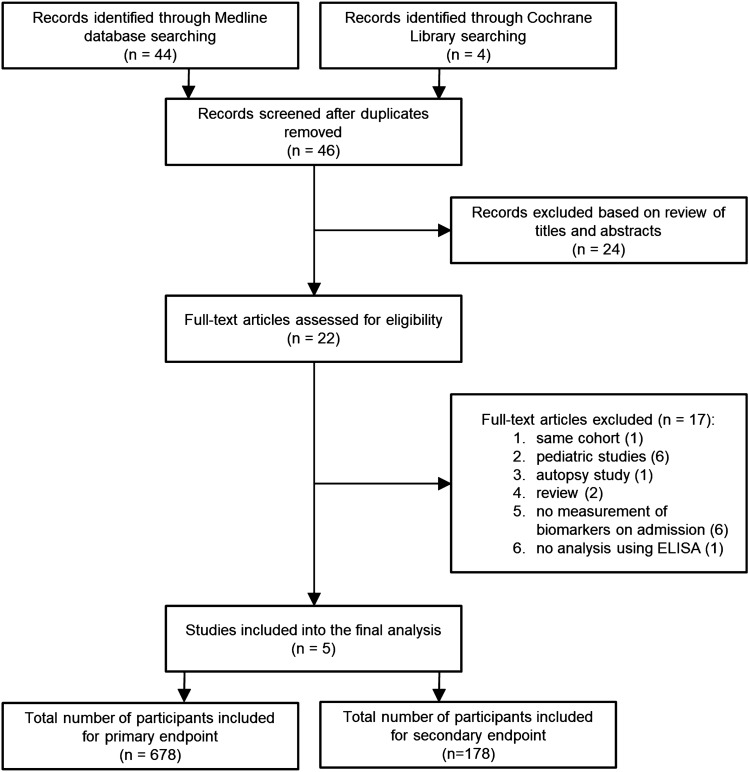
Methods: A systematic search across Cochrane Central Register of Controlled Trials and MEDLINE databases (1966 to February 2022) for studies on PSP published in English using 'pancreatic stone protein', 'PSP', 'regenerative protein', 'lithostatin' combined with 'infection' and 'sepsis' found 46 records. The search was restricted to the five trials that measured PSP using the enzyme-linked immunosorbent assay technique (ELISA). We used Bayesian hierarchical regression models for pooled estimates and to predict mortality or disease severity using PSP, C-Reactive Protein (CRP) and procalcitonin (PCT) as main predictor. We used statistical discriminative measures, such as the area under the receiver operating characteristic curve (AUC) and classification plots.
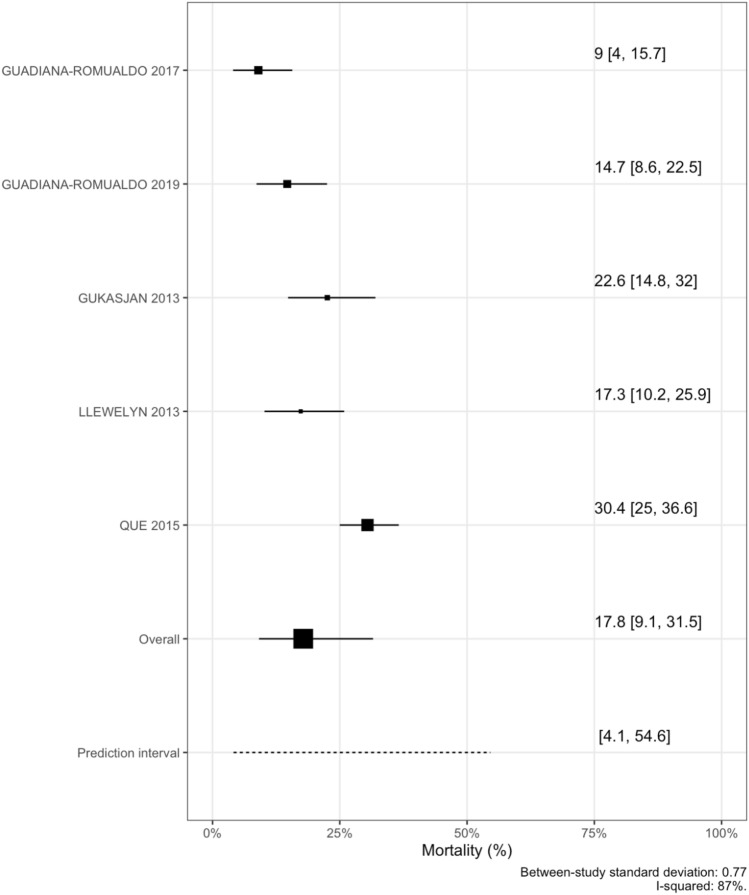
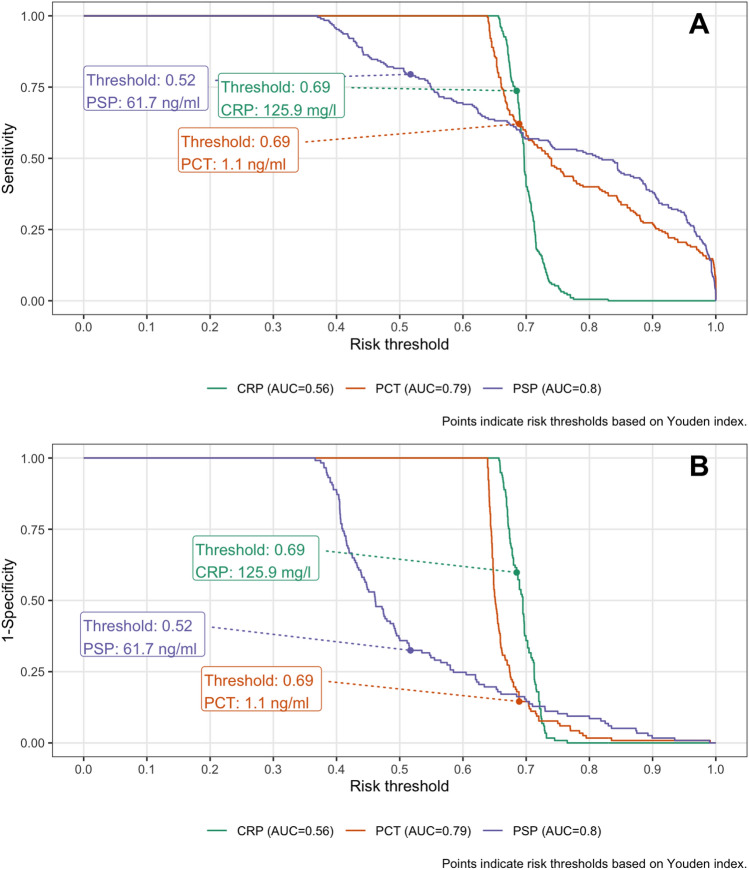
Results: Among the 678 patients included, the pooled ICU mortality was 17.8% (95% prediction interval 4.1% to 54.6%) with a between-study heterogeneity (I-squared 87%). PSP was strongly associated with ICU mortality (OR = 2.7, 95% credible interval (CrI) [1.3-6.0] per one standard deviation increase; age, gender and sepsis severity adjusted OR = 1.5, 95% CrI [0.98-2.8]). The AUC was 0.69 for PSP 95% confidence interval (CI) [0.64-0.74], 0.61 [0.56-0.66] for PCT and 0.52 [0.47-0.57] for CRP. The sensitivity was 0.96, 0.52, 0.30 for risk thresholds 0.1, 0.2 and 0.3; respective false positive rate values were 0.84, 0.25, 0.10.
Conclusions: We found that PSP showed a very good discriminative ability for both investigated study endpoints ICU mortality and infection severity; better in comparison to CRP, similar to PCT. Combinations of biomarkers did not improve their predictive ability.
Keywords: Biomarker; Infection; Mortality; PSP; Pancreatic stone protein.
© 2023. The Author(s).
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures

References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–377. doi: 10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Seppälä TT, Zimmerman JW, Suri R, Zlomke H, Ivey GD, Szabolcs A, Shubert CR, Cameron JL, Burns WR, Lafaro KJ, et al. Precision medicine in pancreatic cancer: patient-derived organoid pharmacotyping is a predictive biomarker of clinical treatment response. Clin Cancer Res. 2022;28:3296–3307. doi: 10.1158/1078-0432.CCR-21-4165. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
