

Enhanced antitumour immunity following neoadjuvant chemoradiotherapy mediates a favourable prognosis in women with resected pancreatic cancer
- PMID: 37709493
- PMCID: PMC10850691
- DOI: 10.1136/gutjnl-2023-330480
Enhanced antitumour immunity following neoadjuvant chemoradiotherapy mediates a favourable prognosis in women with resected pancreatic cancer
Abstract
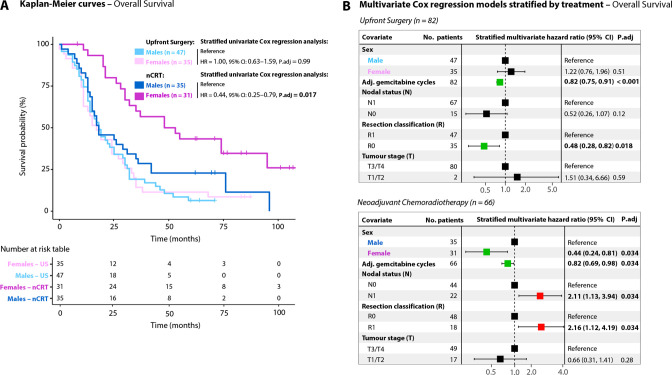
Background: This study investigates sex disparities in clinical outcomes and tumour immune profiles in patients with pancreatic ductal adenocarcinoma (PDAC) who underwent upfront resection or resection preceded by gemcitabine-based neoadjuvant chemoradiotherapy (nCRT).
Methods: Patients originated from the PREOPANC randomised controlled trial. Upfront surgery was performed in 82 patients, and 66 received nCRT before resection. The impact of sex on overall survival (OS) was investigated using Cox proportional hazards models. The immunological landscape within the tumour microenvironment (TME) was mapped using transcriptomic and spatial proteomic profiling.
Results: The 5-year OS rate differed between the sexes following resection preceded by nCRT, with 43% for women compared with 22% for men. In multivariate analysis, the female sex was a favourable independent prognostic factor for OS only in the nCRT group (HR 0.19; 95% CI 0.07 to 0.52). Multivariate heterogeneous treatment effects analysis revealed a significant interaction between sex and treatment, implying increased nCRT efficacy among women with resected PDAC. The TME of women contained fewer protumoural CD163+MRC1+M2 macrophages than that of men after nCRT, as indicated by transcriptomic and validated using spatial proteomic profiling.
Conclusion: PDAC tumours of women are more sensitive to gemcitabine-based nCRT, resulting in longer OS after resection compared with men. This may be due to enhanced immunity impeding the infiltration of protumoral M2 macrophages into the TME. Our findings highlight the importance of considering sex disparities and mitigating immunosuppressive macrophage polarisation for personalised PDAC treatment.
Keywords: CHEMOTHERAPY; MACROPHAGES; PANCREATIC CANCER; PANCREATIC SURGERY; RADIOTHERAPY.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





Comment in
-
Female advantage in neoadjuvant pancreatic cancer therapy: is it down to macrophages?Gut. 2024 Jan 5;73(2):214-215. doi: 10.1136/gutjnl-2023-330830. Gut. 2024. PMID: 37813566 No abstract available.
Similar articles
-
Metformin boosts antitumor immunity and improves prognosis in upfront resected pancreatic cancer: an observational study.J Natl Cancer Inst. 2024 Aug 1;116(8):1374-1383. doi: 10.1093/jnci/djae070. J Natl Cancer Inst. 2024. PMID: 38530777 Free PMC article. Clinical Trial.
-
Intraoperative Radiotherapy in the Era of Intensive Neoadjuvant Chemotherapy and Chemoradiotherapy for Pancreatic Adenocarcinoma.Am J Clin Oncol. 2018 Jun;41(6):607-612. doi: 10.1097/COC.0000000000000336. Am J Clin Oncol. 2018. PMID: 27740973
-
Survival outcomes of neoadjuvant therapy followed by radical resection versus upfront surgery for stage I-III pancreatic ductal adenocarcinoma: a retrospective cohort study.Int J Surg. 2023 Jun 1;109(6):1573-1583. doi: 10.1097/JS9.0000000000000425. Int J Surg. 2023. PMID: 37132194 Free PMC article.
-
A single center experience in resectable pancreatic ductal adenocarcinoma : the limitations of the surgery-first approach. Critical review of the literature and proposals for practice update.Acta Gastroenterol Belg. 2017 Oct-Dec;80(4):451-461. Acta Gastroenterol Belg. 2017. Retraction in: Acta Gastroenterol Belg. 2018 Apr-Jun;81(2):358. PMID: 29560639 Retracted. Review.
-
Neoadjuvant Treatment in Patients With Resectable and Borderline Resectable Pancreatic Cancer.Front Oncol. 2020 Jan 31;10:41. doi: 10.3389/fonc.2020.00041. eCollection 2020. Front Oncol. 2020. PMID: 32083002 Free PMC article.
Cited by
-
Enhanced Complement Expression in the Tumor Microenvironment Following Neoadjuvant Therapy: Implications for Immunomodulation and Survival in Pancreatic Ductal Adenocarcinoma.Res Sq [Preprint]. 2024 May 13:rs.3.rs-4104258. doi: 10.21203/rs.3.rs-4104258/v1. Res Sq. 2024. Update in: NPJ Precis Oncol. 2025 Mar 3;9(1):58. doi: 10.1038/s41698-025-00848-2. PMID: 38798691 Free PMC article. Updated. Preprint.
-
Cancer Vaccination and Immune-Based Approaches in Pancreatic Cancer.Cancers (Basel). 2025 Jul 15;17(14):2356. doi: 10.3390/cancers17142356. Cancers (Basel). 2025. PMID: 40723238 Free PMC article. Review.
-
Exogenous or in situ vaccination to trigger clinical responses in pancreatic cancer.Carcinogenesis. 2024 Nov 22;45(11):826-835. doi: 10.1093/carcin/bgae065. Carcinogenesis. 2024. PMID: 39514560 Review.
-
Single-cell spatial proteomics of non-relapse small cell lung cancer identifies tumor microenvironment determinants of survival.Cell Biol Toxicol. 2025 Jun 17;41(1):106. doi: 10.1007/s10565-025-10056-0. Cell Biol Toxicol. 2025. PMID: 40526293 Free PMC article.
-
Role of radiotherapy in surgical approaches to pancreatic cancer treatment: A narrative review.Ann Gastroenterol Surg. 2025 Mar 7;9(3):418-428. doi: 10.1002/ags3.70012. eCollection 2025 May. Ann Gastroenterol Surg. 2025. PMID: 40385329 Free PMC article. Review.
References
-
- Neoptolemos JP, Palmer DH, Ghaneh P, et al. . Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet 2017;389:1011–24. 10.1016/S0140-6736(16)32409-6 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous