

MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial
- PMID: 37709999
- PMCID: PMC10579091
- DOI: 10.1038/s41591-023-02565-4
MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial
Erratum in
-
Author Correction: MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial.Nat Med. 2024 Nov;30(11):3382. doi: 10.1038/s41591-024-03331-w. Nat Med. 2024. PMID: 39375459 Free PMC article. No abstract available.
Abstract
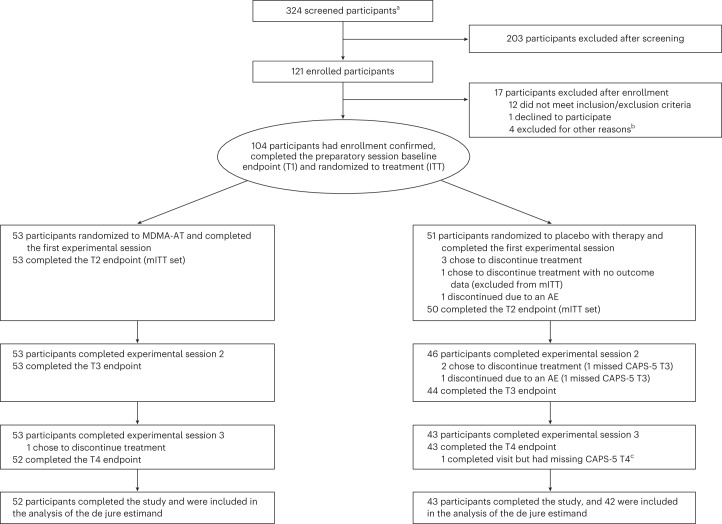
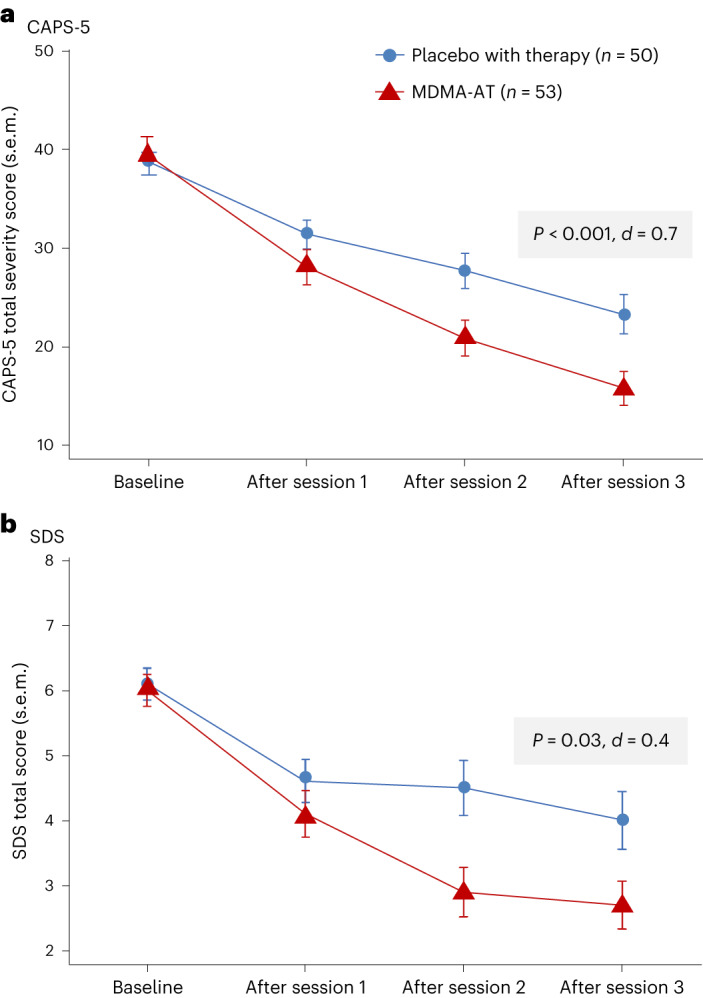
This multi-site, randomized, double-blind, confirmatory phase 3 study evaluated the efficacy and safety of 3,4-methylenedioxymethamphetamine-assisted therapy (MDMA-AT) versus placebo with identical therapy in participants with moderate to severe post-traumatic stress disorder (PTSD). Changes in Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) total severity score (primary endpoint) and Sheehan Disability Scale (SDS) functional impairment score (key secondary endpoint) were assessed by blinded independent assessors. Participants were randomized to MDMA-AT (n = 53) or placebo with therapy (n = 51). Overall, 26.9% (28/104) of participants had moderate PTSD, and 73.1% (76/104) of participants had severe PTSD. Participants were ethnoracially diverse: 28 of 104 (26.9%) identified as Hispanic/Latino, and 35 of 104 (33.7%) identified as other than White. Least squares (LS) mean change in CAPS-5 score (95% confidence interval (CI)) was -23.7 (-26.94, -20.44) for MDMA-AT versus -14.8 (-18.28, -11.28) for placebo with therapy (P < 0.001, d = 0.7). LS mean change in SDS score (95% CI) was -3.3 (-4.03, -2.60) for MDMA-AT versus -2.1 (-2.89, -1.33) for placebo with therapy (P = 0.03, d = 0.4). Seven participants had a severe treatment emergent adverse event (TEAE) (MDMA-AT, n = 5 (9.4%); placebo with therapy, n = 2 (3.9%)). There were no deaths or serious TEAEs. These data suggest that MDMA-AT reduced PTSD symptoms and functional impairment in a diverse population with moderate to severe PTSD and was generally well tolerated. ClinicalTrials.gov identifier: NCT04077437 .
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
J.M.M. has received research support from MAPS; grants/contracts from the Veterans Administration (Merit Award) and the FDA (Research Award); has received royalties/licenses from UCLA (for a patent licensed to UCSF for cell screening); has received payment/honoraria from Stanford (for lecturing to undergraduate students) and Johns Hopkins (for presenting grand rounds); has a patent licensed to UCSF for cell screening; has been a reviewer for NIAAA CTN; has been a member of CA DOJ RAP; and has been a grant reviewer for the Australian Medical Research Council. M.O.G.: Aguazul-Bluewater, Inc has received research support from MAPS PBC and payments from Cybin (training and consultation), from Horizons Conference and from Naropa University. B.v.d.K. has received royalties from Penguin Random House (book,
Figures
Comment in
-
Expectancy Effects Cannot Be Neglected in MDMA-Assisted Therapy Research.ACS Chem Neurosci. 2023 Dec 6;14(23):4062-4063. doi: 10.1021/acschemneuro.3c00692. Epub 2023 Nov 15. ACS Chem Neurosci. 2023. PMID: 37967550 Free PMC article. No abstract available.
References
-
- US Department of Veteran Affairs. PTSD: National Center for PTSD. How common is PTSD in adults? (https://www.ptsd.va.gov/understand/common/common_adults.asp).
