

Financial hardship associated with catastrophic out-of-pocket spending tied to primary care services in low- and lower-middle-income countries: findings from a modeling study
- PMID: 37710266
- PMCID: PMC10503078
- DOI: 10.1186/s12916-023-02957-w
Financial hardship associated with catastrophic out-of-pocket spending tied to primary care services in low- and lower-middle-income countries: findings from a modeling study
Abstract
Background: Financial risk protection (FRP) is a key component of universal health coverage (UHC): all individuals must be able to obtain the health services they need without experiencing financial hardship. In many low-income and lower-middle-income countries, however, the health system fails to provide sufficient protection against high out-of-pocket (OOP) spending on health services. In 2018, OOP health spending comprised approximately 40% of current health expenditures in low-income and lower-middle-income countries.
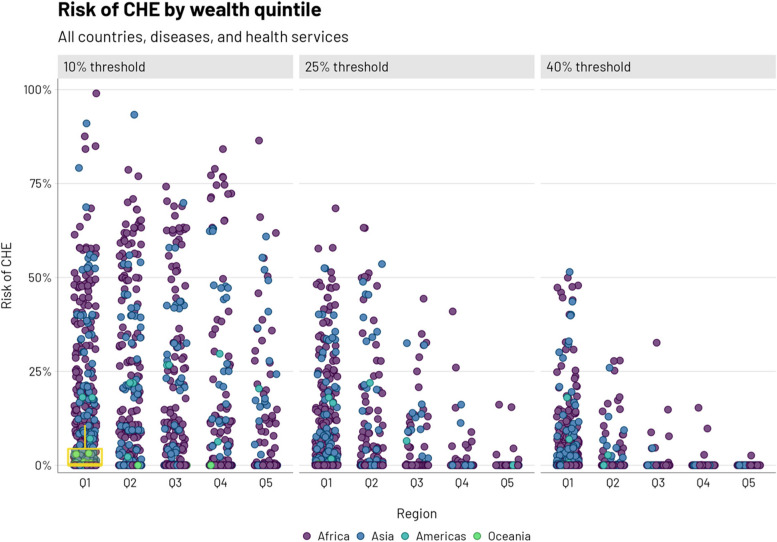
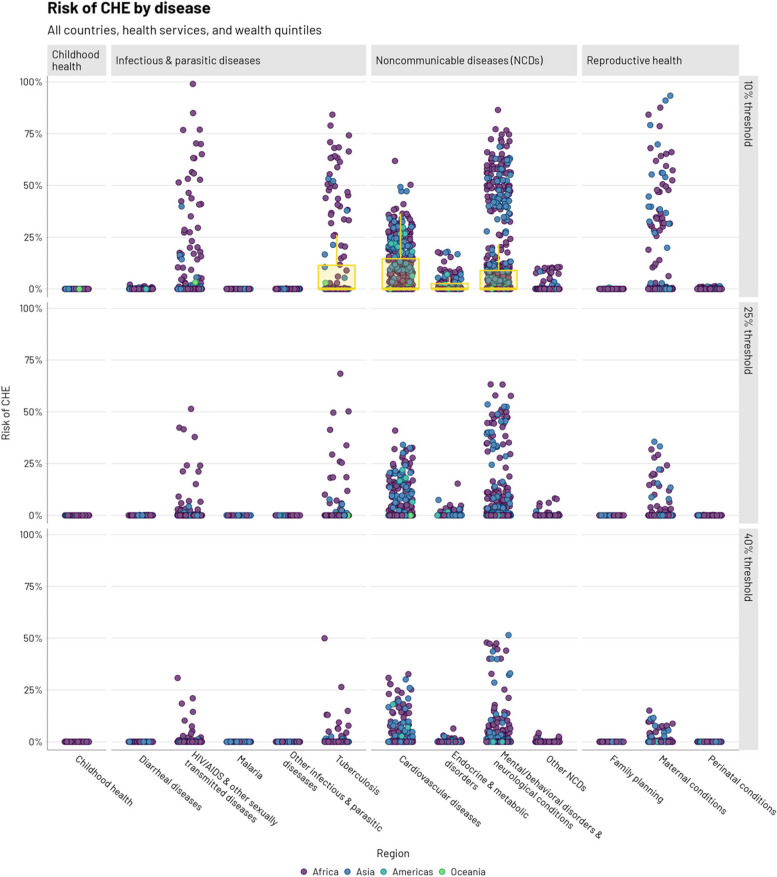
Methods: We model the household risk of catastrophic health expenditures (CHE), conditional on having a given disease or condition-defined as OOP health spending that exceeds a threshold percentage (10, 25, or 40%) of annual income-for 29 health services across 13 disease categories (e.g., diarrheal diseases, cardiovascular diseases) in 34 low-income and lower-middle-income countries. Health services were included in the analysis if delivered at the primary care level and part of the Disease Control Priorities, 3rd edition "highest priority package." Data were compiled from several publicly available sources, including national health accounts, household surveys, and the published literature. A risk of CHE, conditional on having disease, was modeled as depending on usage, captured through utilization indicators; affordability, captured via the level of public financing and OOP health service unit costs; and income.
Results: Across all countries, diseases, and health services, the risk of CHE (conditional on having a disease) would be concentrated among poorer quintiles (6.8% risk in quintile 1 vs. 1.3% in quintile 5 using a 10% CHE threshold). The risk of CHE would be higher for a few disease areas, including cardiovascular disease and mental/behavioral disorders (7.8% and 9.8% using a 10% CHE threshold), while lower risks of CHE were observed for lower cost services.
Conclusions: Insufficient FRP stands as a major barrier to achieving UHC, and risk of CHE is a major problem for health systems in low-income and lower-middle-income countries. Beyond its threat to the financial stability of households, CHE may also lead to worse health outcomes, especially among the poorest for whom both ill health and financial risk are most severe. Modeling the risk of CHE associated with specific disease areas and services can help policymakers set progressive health sector priorities. Decision-makers could explicitly include FRP as a criterion for consideration when assessing the health interventions for inclusion in national essential benefit packages.
Keywords: Catastrophic health expenditures; Financial risk protection; Out-of-pocket medical costs; Priority setting; Universal health coverage.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- UN General Assembly resolution 70/1 . Transforming our world: the 2030 Agenda for Sustainable Development. 2015.
-
- World Bank. World Development Indicators. DataBank n.d. https://databank.worldbank.org/source/world-development-indicators. Accessed 5 Nov 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
