

Identification of a ferroptosis-related gene signature predicting recurrence in stage II/III colorectal cancer based on machine learning algorithms
- PMID: 37711170
- PMCID: PMC10498388
- DOI: 10.3389/fphar.2023.1260697
Identification of a ferroptosis-related gene signature predicting recurrence in stage II/III colorectal cancer based on machine learning algorithms
Abstract
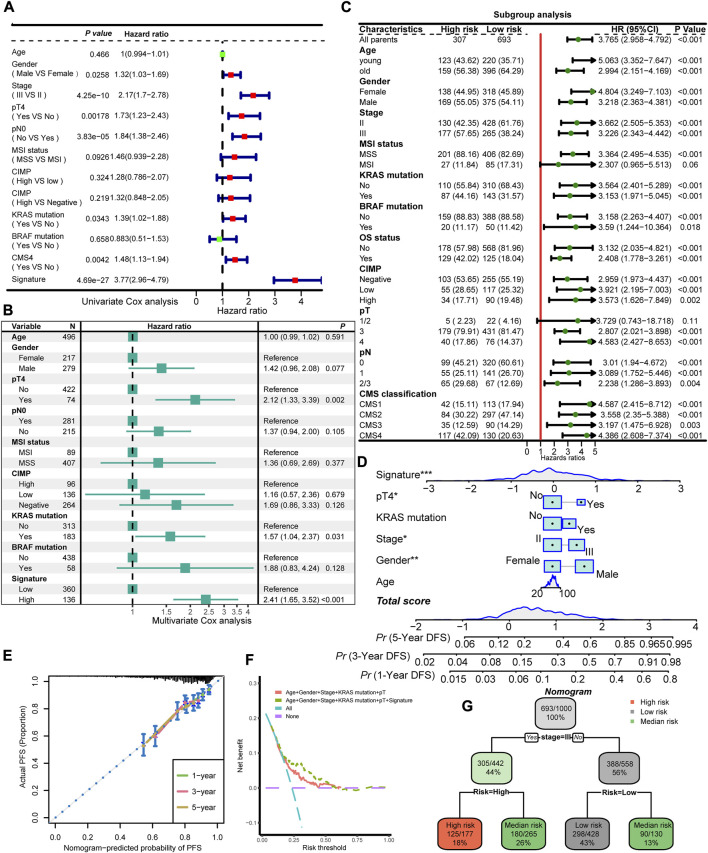
Background: Colorectal cancer (CRC) is one of the most prevalent cancer types globally. A survival paradox exists due to the inherent heterogeneity in stage II/III CRC tumor biology. Ferroptosis is closely related to the progression of tumors, and ferroptosis-related genes can be used as a novel biomarker in predicting cancer prognosis. Methods: Ferroptosis-related genes were retrieved from the FerrDb and KEGG databases. A total of 1,397 samples were enrolled in our study from nine independent datasets, four of which were integrated as the training dataset to train and construct the model, and validated in the remaining datasets. We developed a machine learning framework with 83 combinations of 10 algorithms based on 10-fold cross-validation (CV) or bootstrap resampling algorithm to identify the most robust and stable model. C-indice and ROC analysis were performed to gauge its predictive accuracy and discrimination capabilities. Survival analysis was conducted followed by univariate and multivariate Cox regression analyses to evaluate the performance of identified signature. Results: The ferroptosis-related gene (FRG) signature was identified by the combination of Lasso and plsRcox and composed of 23 genes. The FRG signature presented better performance than common clinicopathological features (e.g., age and stage), molecular characteristics (e.g., BRAF mutation and microsatellite instability) and several published signatures in predicting the prognosis of the CRC. The signature was further stratified into a high-risk group and low-risk subgroup, where a high FRG signature indicated poor prognosis among all collected datasets. Sensitivity analysis showed the FRG signature remained a significant prognostic factor. Finally, we have developed a nomogram and a decision tree to enhance prognosis evaluation. Conclusion: The FRG signature enabled the accurate selection of high-risk stage II/III CRC population and helped optimize precision treatment to improve their clinical outcomes.
Keywords: ferroptosis-related gene; machine learning; prognosis; stage II/III colorectal cancer; tumor heterogeneity.
Copyright © 2023 Wang, Ma, Teng, Man, Zhang, Liu, Zhang, Chong, Chen and Lu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
Machine learning-based analysis identifies a 13-gene prognostic signature to improve the clinical outcomes of colorectal cancer.J Gastrointest Oncol. 2024 Oct 31;15(5):2100-2116. doi: 10.21037/jgo-24-325. Epub 2024 Oct 24. J Gastrointest Oncol. 2024. PMID: 39554586 Free PMC article.
-
A Ferroptosis-Related Gene Signature Identified as a Novel Prognostic Biomarker for Colon Cancer.Front Genet. 2021 Jul 1;12:692426. doi: 10.3389/fgene.2021.692426. eCollection 2021. Front Genet. 2021. PMID: 34276794 Free PMC article.
-
Identification and validation of a novel ferroptosis-related gene signature for prognosis and potential therapeutic target prediction in cholangiocarcinoma.Front Immunol. 2023 Jan 17;13:1051273. doi: 10.3389/fimmu.2022.1051273. eCollection 2022. Front Immunol. 2023. PMID: 36733386 Free PMC article.
-
Identification of an EMT-related Gene Signature Predicting Recurrence in Stage II/III Colorectal Cancer: A Retrospective Study in 1780 Patients.Ann Surg. 2022 Nov 1;276(5):897-904. doi: 10.1097/SLA.0000000000005644. Epub 2022 Jul 26. Ann Surg. 2022. PMID: 35880752
-
A Novel Prognosis Signature Based on Ferroptosis-Related Gene DNA Methylation Data for Lung Squamous Cell Carcinoma.J Oncol. 2022 Sep 12;2022:9103259. doi: 10.1155/2022/9103259. eCollection 2022. J Oncol. 2022. PMID: 36131791 Free PMC article.
Cited by
-
A novel gene signature for predicting outcome in colorectal cancer patients based on tumor cell-endothelial cell interaction via single-cell sequencing and machine learning.Heliyon. 2025 Jan 24;11(3):e42237. doi: 10.1016/j.heliyon.2025.e42237. eCollection 2025 Feb 15. Heliyon. 2025. PMID: 39944338 Free PMC article.
-
Effectiveness of Artificial Intelligence Models in Predicting Lung Cancer Recurrence: A Gene Biomarker-Driven Review.Cancers (Basel). 2025 Jun 5;17(11):1892. doi: 10.3390/cancers17111892. Cancers (Basel). 2025. PMID: 40507370 Free PMC article. Review.
-
Exploration and validation of the prognostic value of mitophagy and mitochondrial dynamics-related genes in cervical cancer.Sci Rep. 2025 Jul 10;15(1):24950. doi: 10.1038/s41598-025-09310-6. Sci Rep. 2025. PMID: 40640353 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials