

Maternal PlGF and umbilical Dopplers predict pregnancy outcomes at diagnosis of early-onset fetal growth restriction
- PMID: 37712421
- PMCID: PMC10503803
- DOI: 10.1172/JCI169199
Maternal PlGF and umbilical Dopplers predict pregnancy outcomes at diagnosis of early-onset fetal growth restriction
Abstract
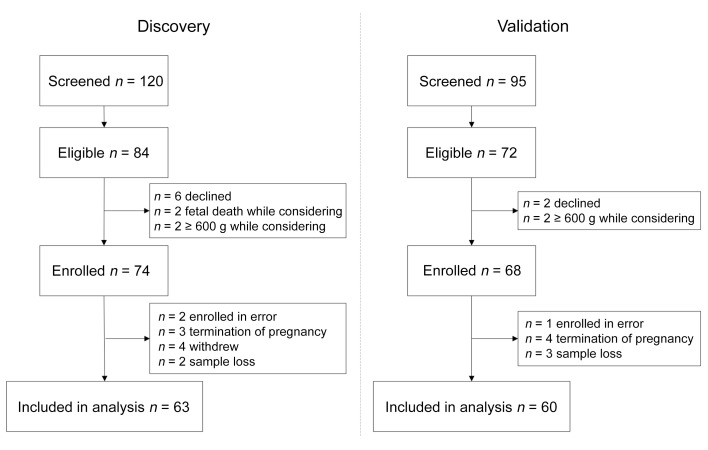
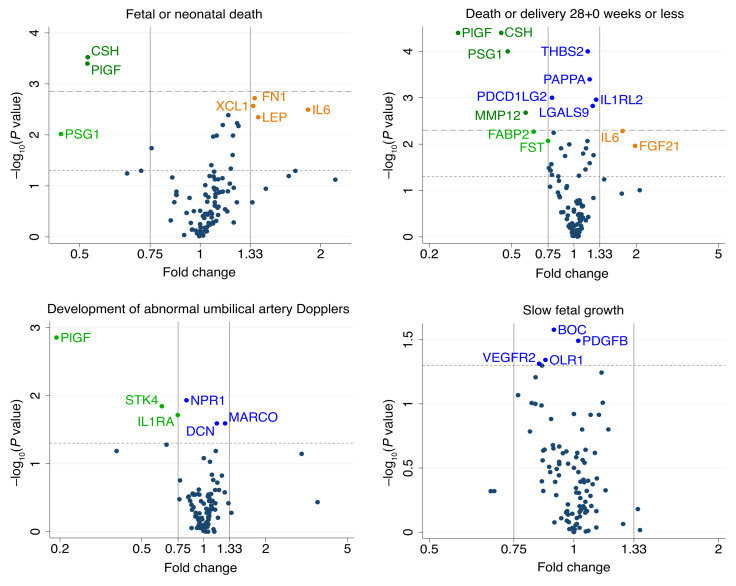
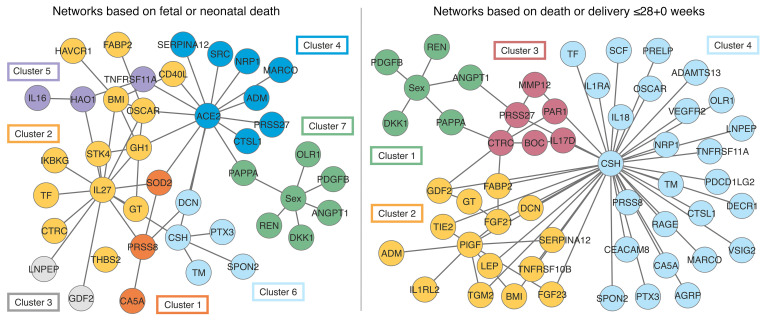
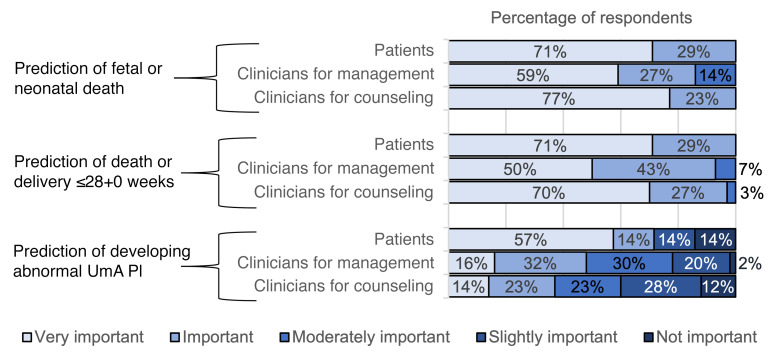
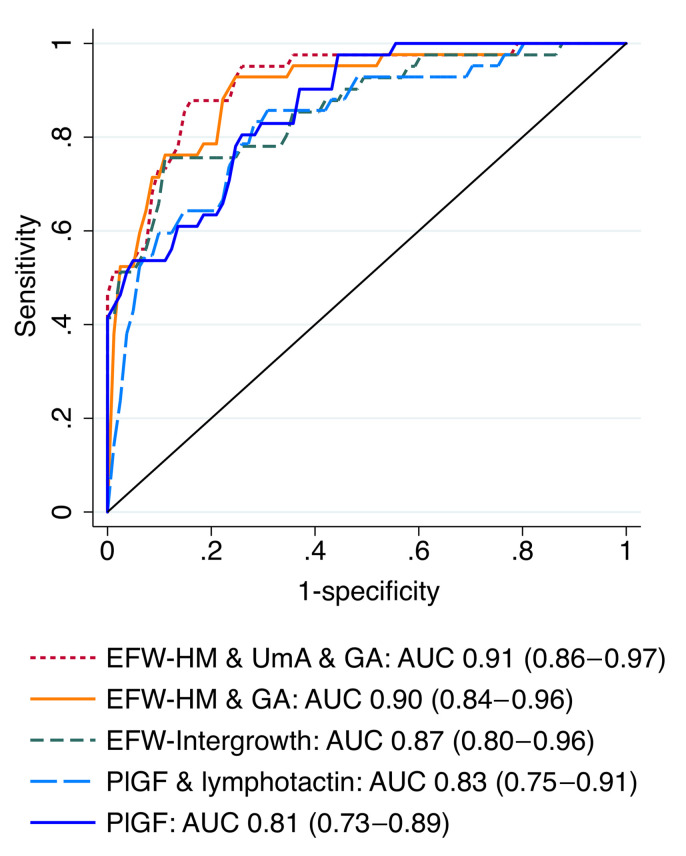
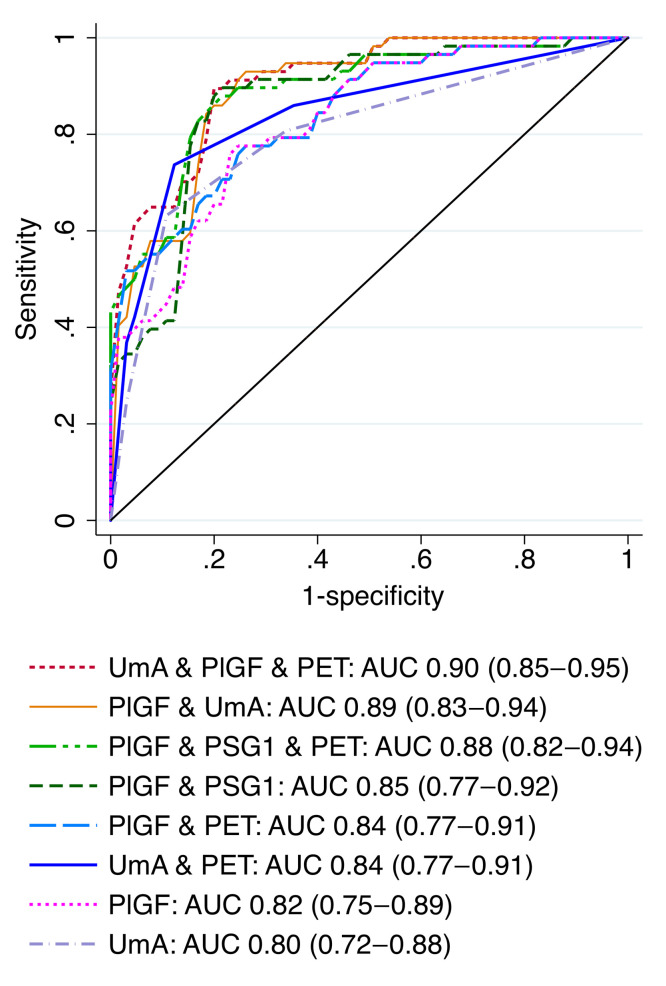
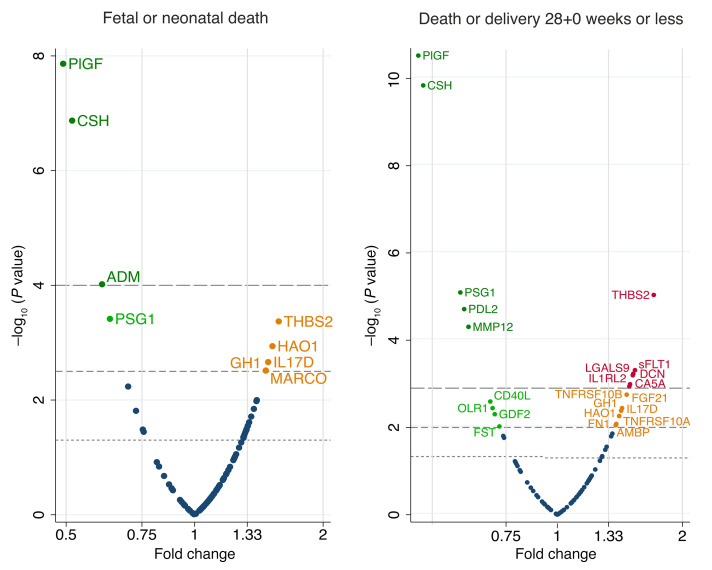
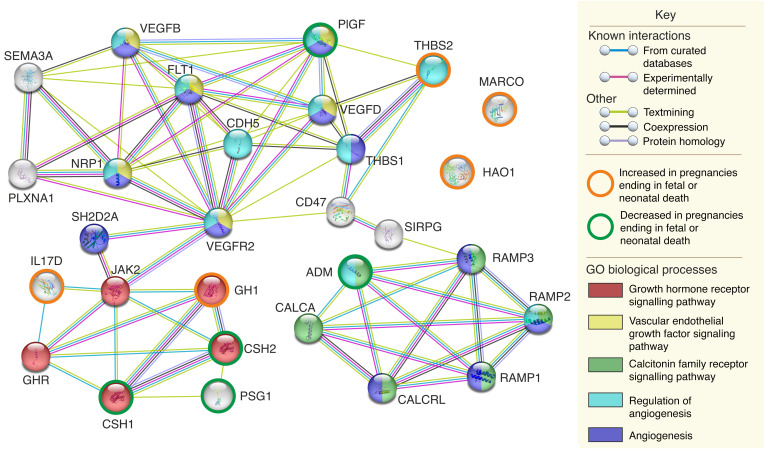
BACKGROUNDSevere, early-onset fetal growth restriction (FGR) causes significant fetal and neonatal mortality and morbidity. Predicting the outcome of affected pregnancies at the time of diagnosis is difficult, thus preventing accurate patient counseling. We investigated the use of maternal serum protein and ultrasound measurements at diagnosis to predict fetal or neonatal death and 3 secondary outcomes: fetal death or delivery at or before 28+0 weeks, development of abnormal umbilical artery (UmA) Doppler velocimetry, and slow fetal growth.METHODSWomen with singleton pregnancies (n = 142, estimated fetal weights [EFWs] below the third centile, less than 600 g, 20+0 to 26+6 weeks of gestation, no known chromosomal, genetic, or major structural abnormalities) were recruited from 4 European centers. Maternal serum from the discovery set (n = 63) was analyzed for 7 proteins linked to angiogenesis, 90 additional proteins associated with cardiovascular disease, and 5 proteins identified through pooled liquid chromatography and tandem mass spectrometry. Patient and clinician stakeholder priorities were used to select models tested in the validation set (n = 60), with final models calculated from combined data.RESULTSThe most discriminative model for fetal or neonatal death included the EFW z score (Hadlock 3 formula/Marsal chart), gestational age, and UmA Doppler category (AUC, 0.91; 95% CI, 0.86-0.97) but was less well calibrated than the model containing only the EFW z score (Hadlock 3/Marsal). The most discriminative model for fetal death or delivery at or before 28+0 weeks included maternal serum placental growth factor (PlGF) concentration and UmA Doppler category (AUC, 0.89; 95% CI, 0.83-0.94).CONCLUSIONUltrasound measurements and maternal serum PlGF concentration at diagnosis of severe, early-onset FGR predicted pregnancy outcomes of importance to patients and clinicians.TRIAL REGISTRATIONClinicalTrials.gov NCT02097667.FUNDINGThe European Union, Rosetrees Trust, Mitchell Charitable Trust.
Keywords: Clinical practice; Diagnostics; Obstetrics/gynecology; Reproductive Biology.
Figures
Comment in
-
Scaling the EVERREST of severe, early-onset fetal growth restriction.J Clin Invest. 2023 Sep 15;133(18):e173563. doi: 10.1172/JCI173563. J Clin Invest. 2023. PMID: 37712422 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
