

Prognosis and management of acute symptomatic seizures: a prospective, multicenter, observational study
- PMID: 37712992
- PMCID: PMC10504169
- DOI: 10.1186/s13613-023-01183-0
Prognosis and management of acute symptomatic seizures: a prospective, multicenter, observational study
Abstract
Background: Acute symptomatic epileptic seizures are frequently seen in neurocritical care. To prevent subsequent unprovoked seizures, long-term treatments with antiseizure medications are often initiated although supporting evidence is lacking. This study aimed at prospectively assessing the risk of unprovoked seizure relapse with respect to the use of antiseizure medications. It was hypothesized that after a first acute symptomatic seizure of structural etiology, the cumulative 12-month risk of unprovoked seizure relapse is ≤ 25%.
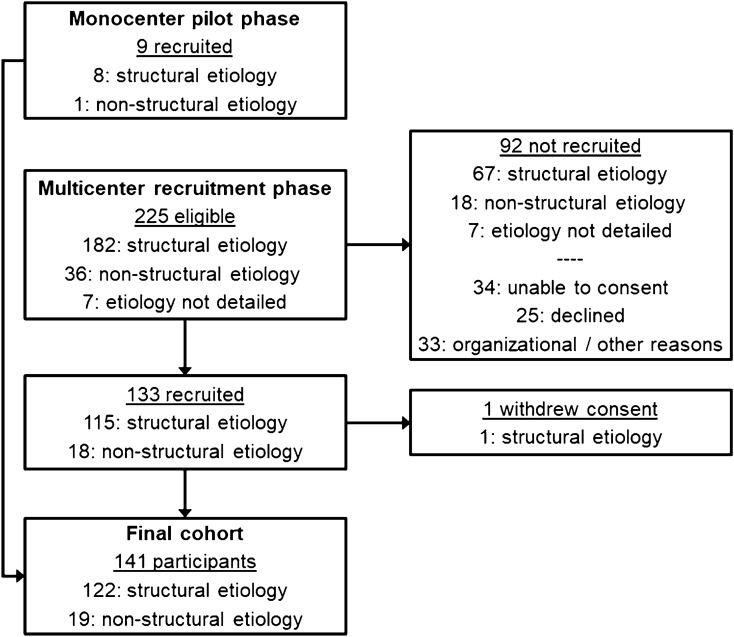
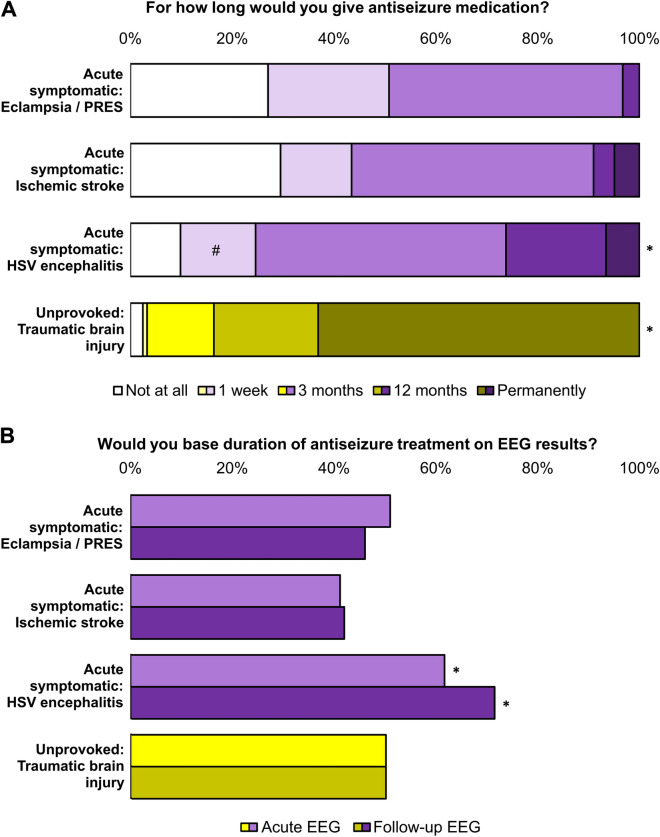
Methods: Inclusion criteria were age ≥ 18 and acute symptomatic first-ever epileptic seizure; patients with status epilepticus were excluded. Using telephone and mail interviews, participants were followed for 12 months after the acute symptomatic first seizure. Primary endpoint was the occurrence and timing of a first unprovoked seizure relapse. In addition, neuro-intensivists in Germany were interviewed about their antiseizure treatment strategies through an anonymous online survey.
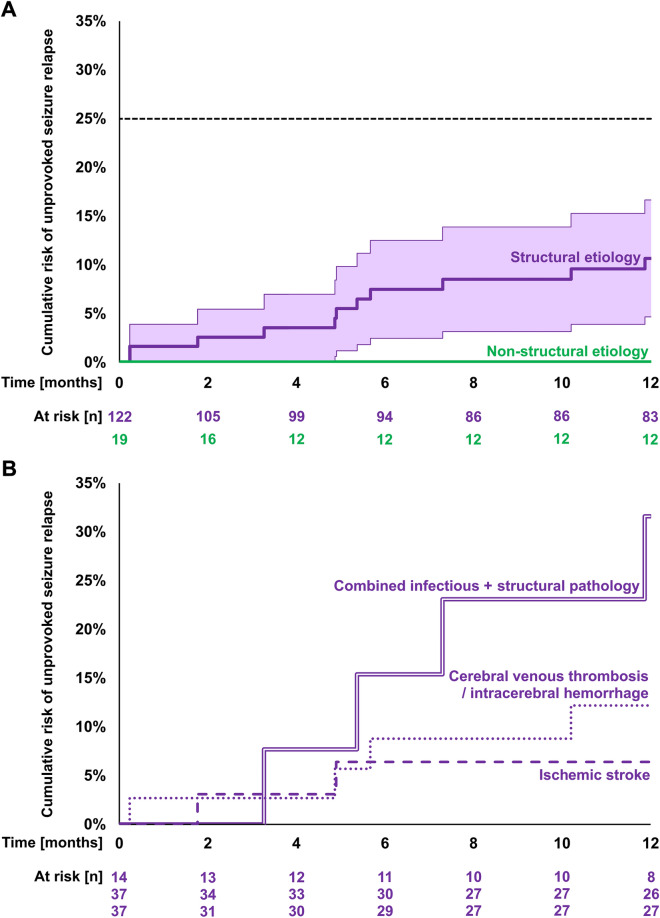
Results: Eleven of 122 participants with structural etiology had an unprovoked seizure relapse, resulting in a cumulative 12-month risk of 10.7% (95%CI, 4.7%-16.7%). None of 19 participants with a non-structural etiology had a subsequent unprovoked seizure. Compared to structural etiology alone, combined infectious and structural etiology was independently associated with unprovoked seizure relapse (OR 11.1; 95%CI, 1.8-69.7). Median duration of antiseizure treatment was 3.4 months (IQR 0-9.3). Seven out of 11 participants had their unprovoked seizure relapse while taking antiseizure medication; longer treatment durations were not associated with decreased risk of unprovoked seizure relapse. Following the non-representative online survey, most neuro-intensivists consider 3 months or less of antiseizure medication to be adequate.
Conclusions: Even in case of structural etiology, acute symptomatic seizures bear a low risk of subsequent unprovoked seizures. There is still no evidence favoring long-term treatments with antiseizure medications. Hence, individual constellations with an increased risk of unprovoked seizure relapse should be identified, such as central nervous system infections causing structural brain damage. However, in the absence of high-risk features, antiseizure medications should be discontinued early to avoid overtreatment.
Keywords: Acute symptomatic seizure; Antiseizure medication; CNS infection; Cerebrovascular accident; Ischemic stroke; Mortality; Secondary seizure prophylaxis; Seizure risk; Structural brain damage; Unprovoked seizure.
© 2023. La Société de Réanimation de Langue Francaise = The French Society of Intensive Care (SRLF).
Conflict of interest statement
JHN received a travel allowance from Eisai; FS received speaker’s honoraria from Ameos, AstraZeneca, Bristol-Myers Squibb, and MD Horizonte; MW received speaker’s honoraria and consultancy fees from Portola/Alexion; AG received speaker’s honoraria from Boehringer Ingelheim, Daiichi Sankyo, Ipsen, Occlutech, and Pfizer, as well as research grants from Merz and Ipsen; MH received speaker’s honoraria and/or consultancy fees from Angelini, Bial, Desitin, Eisai, Jazz, Neuraxpharm, UCB, and Zogenix. All other authors declare that they have no competing interests.
Figures

References
-
- Beghi E, Carpio A, Forsgren L, Hesdorffer DC, Malmgren K, Sander JW, et al. Recommendation for a definition of acute symptomatic seizure. Epilepsia. 2010;51(4):671–675. - PubMed
-
- Vorderwülbecke BJ, Lichtner G, von Dincklage F, Holtkamp M. Acute antiepileptic drug use in intensive care units. J Neurol. 2018;265(12):2841–2850. - PubMed
-
- Zöllner JP, Konczalla J, Stein M, Roth C, Krakow K, Kaps M, et al. Acute symptomatic seizures in intracerebral and subarachnoid hemorrhage: a population study of 19,331 patients. Epilepsy Res. 2020;161:106286. - PubMed
-
- Lindgren E, Silvis SM, Hiltunen S, Heldner MR, Serrano F, de Scisco M, et al. Acute symptomatic seizures in cerebral venous thrombosis. Neurology. 2020;95(12):e1706–e1715. - PubMed
Grants and funding
- Young Researcher Promotion Award/Deutsche Gesellschaft für Neurointensiv- und -Notfallmedizin DGNI
- 2020/Deutsche Gesellschaft für Neurointensiv- und -Notfallmedizin DGNI
- Clinical Studies Program/Medizinische Fakultät der Albert-Ludwigs-Universität Freiburg
- 3091332005/Medizinische Fakultät der Albert-Ludwigs-Universität Freiburg
- Köln Fortune Program/Faculty of Medicine, University of Cologne
LinkOut - more resources
Full Text Sources
