

Impact of Concomitant Cardiovascular Therapies on Efficacy and Safety of Relugolix vs Leuprolide: Subgroup Analysis from HERO Study in Advanced Prostate Cancer
- PMID: 37713020
- PMCID: PMC10567896
- DOI: 10.1007/s12325-023-02634-7
Impact of Concomitant Cardiovascular Therapies on Efficacy and Safety of Relugolix vs Leuprolide: Subgroup Analysis from HERO Study in Advanced Prostate Cancer
Abstract
Introduction: Cardiovascular (CV) events are the leading cause of death in prostate cancer. Men with prostate cancer are likely to have CV risk factors and use CV-related concomitant medications. In the phase 3 HERO study, a 54% lower incidence of major adverse cardiac events was reported in men treated with the oral gonadotropin-releasing hormone (GnRH) receptor antagonist, relugolix, vs leuprolide. Herein, we characterize the impact of concomitant CV therapies on efficacy and safety in the HERO study.
Methods: In HERO, 930 men with advanced prostate cancer (APC) were randomized 2:1 and treated with relugolix (120 mg orally once daily; after single 360 mg loading dose) or leuprolide (injections every 3 months) for 48 weeks. Subgroups analyzed included men who received antihypertensives, antithrombotics, or lipid-modifying therapies (LMAs), as well as the most common drug classes (> 10%) and single most common agent within each class. Assessments included sustained testosterone suppression to castrate levels (< 50 ng/dL) through 48 weeks and safety.
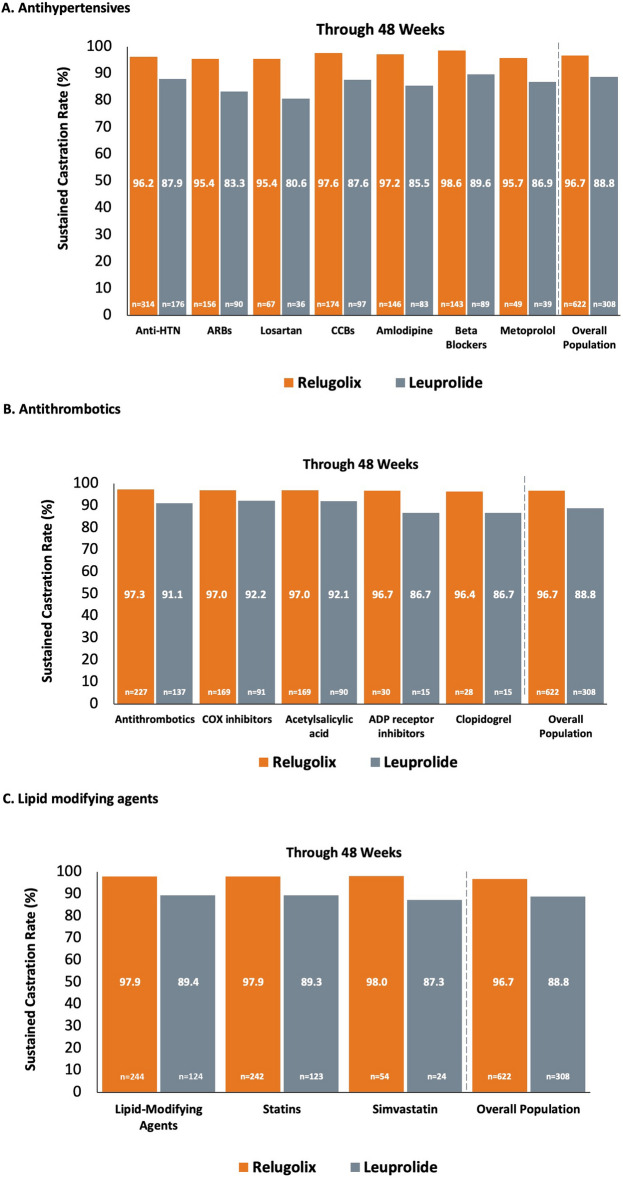
Results: Antihypertensives, antithrombotics, and LMAs were utilized by 52.7%, 39.1%, and 39.6% of men in HERO, respectively. In the main subgroups, point estimates for sustained castration rates were generally consistent with overall estimates of relugolix and leuprolide observed in the overall population. Sustained castration rates were also mostly consistent for men taking the most common drug classes and individual agents in each class (losartan [n = 103]: relugolix, 95.4% vs leuprolide, 80.6%; amlodipine [n = 229]: 97.2% vs 85.5%; metoprolol [n = 88]: 95.7% vs 86.9%; acetylsalicylic acid [n = 259]: 97.0% vs 92.1%; clopidogrel [n = 43]: 96.4% vs 86.7%; simvastatin [n = 78]: 98.0% vs 87.3%). Incidence and types of adverse events (AEs) among men who received these medications were mostly consistent with overall population results, with some increases in grade ≥ 3 and fatal AEs.
Conclusion: Relugolix suppressed testosterone and was generally well tolerated when given with concomitant CV agents.
Trial registration: Clinical Trial ID NCT03085095.
Prior presentation: Data presented at 15th Annual Genitourinary Cancers Symposium; February 17-19, 2022, San Francisco, CA, USA [Abstract 101, Poster board E11]. The published abstract from this presentation can be found at https://ascopubs.org/doi/10.1200/JCO.2022.40.6_suppl.101 .
Keywords: Cardiovascular agents; Leuprolide; Prostate cancer; Relugolix.
© 2023. The Author(s).
Conflict of interest statement
Neal D. Shore—Consulting or Advisory Role: Bayer, Janssen Scientific Affairs, Dendreon, Tolmar, Ferring, Medivation/Astellas, Amgen, Pfizer, AstraZeneca, Genentech, Myovant Sciences. Speakers’ Bureau: Janssen, Bayer, Dendreon. Bryan A. Mehlhaff—Honoraria, travel, and accommodation expenses, and acted as an advisor/consultant for Astellas, Amgen, Bayer, Janssen, and Pfizer; and has received grants/funding from Astellas, Bayer, Janssen, and Pfizer. Michael S. Cookson—Honoraria: Merck, Janssen Biotech, Bayer, Astellas Pharma, Myovant Sciences. Consulting or Advisory Role: Merck, Janssen Biotech, MDxHealth, Bayer, Astellas Pharma, Myovant Sciences, TesoRx Pharma, Genomic Health, Ferring Pharmaceuticals, Precision Biopsy. Daniel R. Saltzstein—No relevant conflicts. Ronald Tutrone—Advisory/Consulting role: Astellas, Pfizer, Myovant, Janssen, Biotechne, Nymox, Dendreon. Speaker: Biotechne, Astellas, Pfizer, Myovant. Bruce Brown; Sophia Lu—Employees of Myovant. Mark Fallick—Employed at Myovant at the time of research and manuscript development. Sarah Hanson—Employee of Pfizer. Fred Saad—Advisory roles for Astellas Pharma, AstraZeneca/MedImmune, Bayer, Janssen Oncology, and Sanofi; has received honoraria from AbbVie, Amgen, Astellas Pharma, AstraZeneca, Bayer, Janssen Oncology, and Sanofi; and has received research funding grants provided to the institution from Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb, Janssen Oncology, Pfizer, and Sanofi.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
