

Population Pharmacokinetics and Exposure-Response with Teclistamab in Patients With Relapsed/Refractory Multiple Myeloma: Results From MajesTEC-1
- PMID: 37713090
- PMCID: PMC10518021
- DOI: 10.1007/s11523-023-00989-z
Population Pharmacokinetics and Exposure-Response with Teclistamab in Patients With Relapsed/Refractory Multiple Myeloma: Results From MajesTEC-1
Abstract
Background: Teclistamab, a B-cell maturation antigen × CD3 bispecific antibody, is approved in patients with relapsed/refractory multiple myeloma (RRMM) who have previously received an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 antibody.
Objective: We report the population pharmacokinetics of teclistamab administered intravenously and subcutaneously (SC) and exposure-response relationships from the phase I/II, first-in-human, open-label, multicenter MajesTEC-1 study.
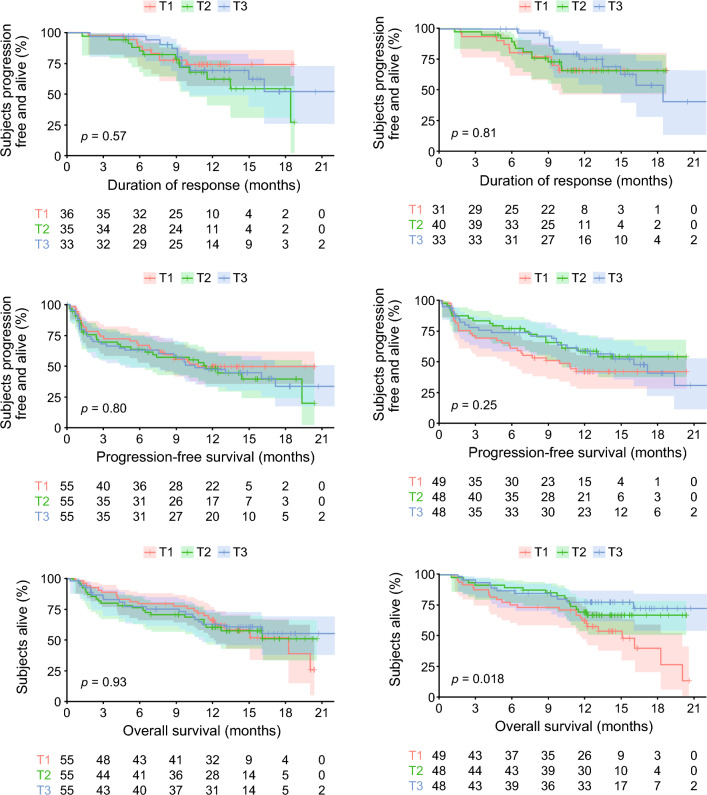
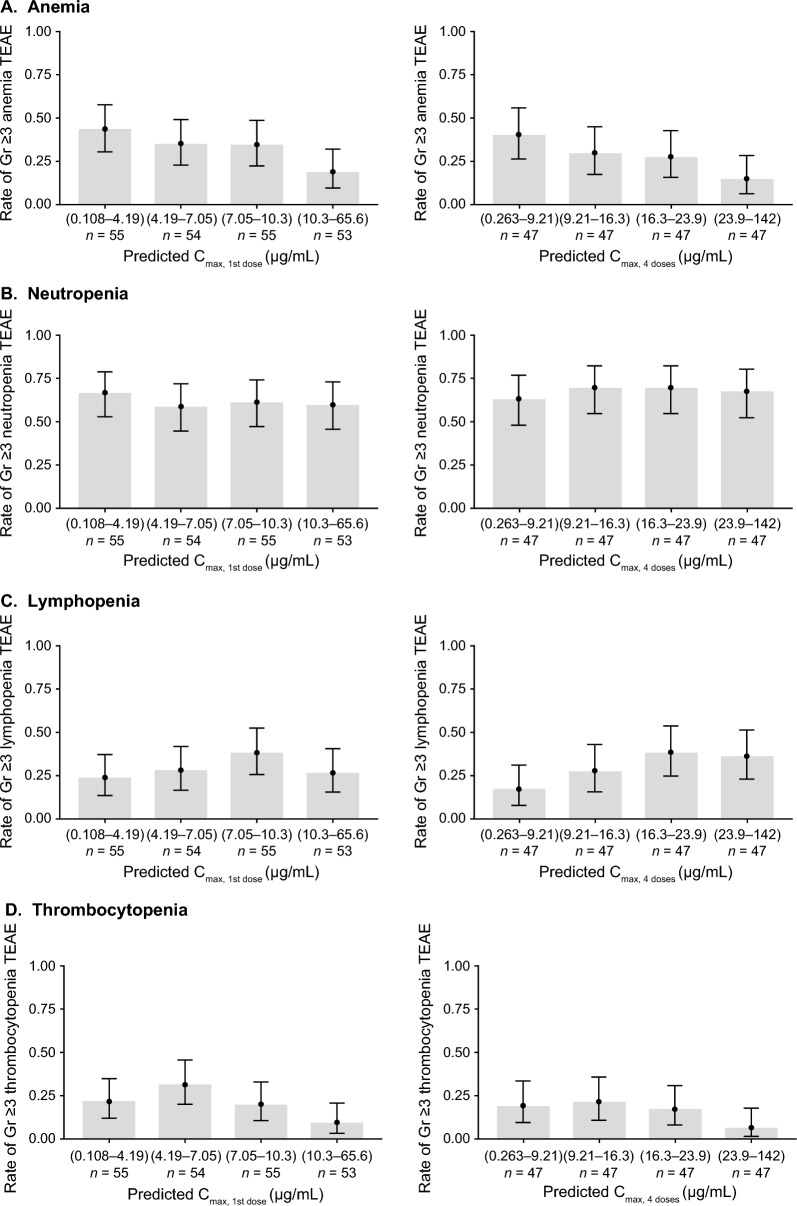
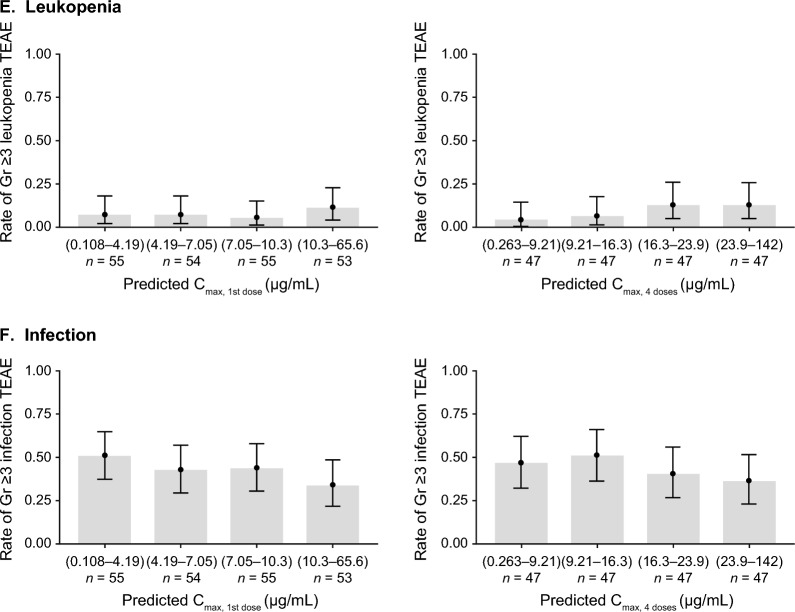
Methods: Phase I of MajesTEC-1 consisted of dose escalation and expansion at the recommended phase II dose (RP2D; 1.5 mg/kg SC weekly, preceded by step-up doses of 0.06 and 0.3 mg/kg); phase II investigated the efficacy of teclistamab RP2D in patients with RRMM. Population pharmacokinetics and the impact of covariates on teclistamab systemic exposure were assessed using a 2-compartment model with first-order absorption for SC and parallel time-independent and time-dependent elimination pathways. Exposure-response analyses were conducted, including overall response rate (ORR), duration of response (DoR), progression-free survival (PFS), overall survival (OS), and the incidence of grade ≥ 3 anemia, neutropenia, lymphopenia, leukopenia, thrombocytopenia, and infection.
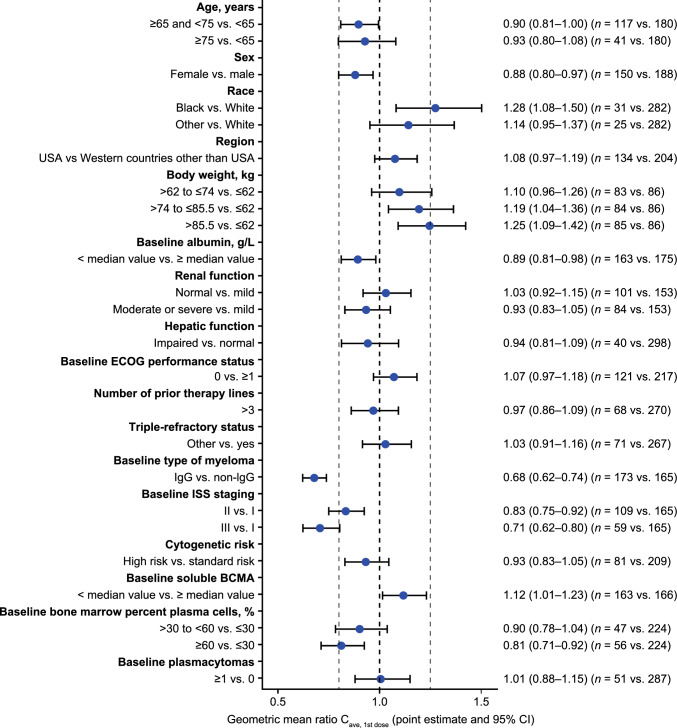
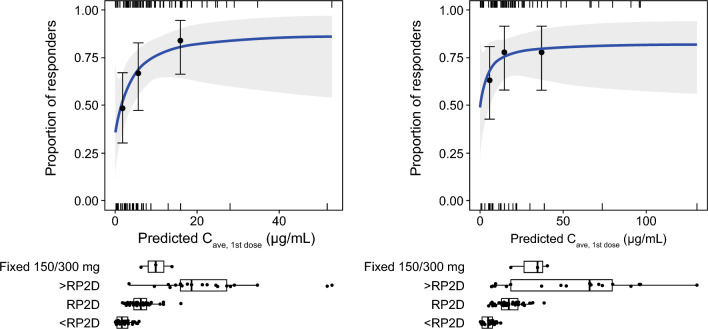
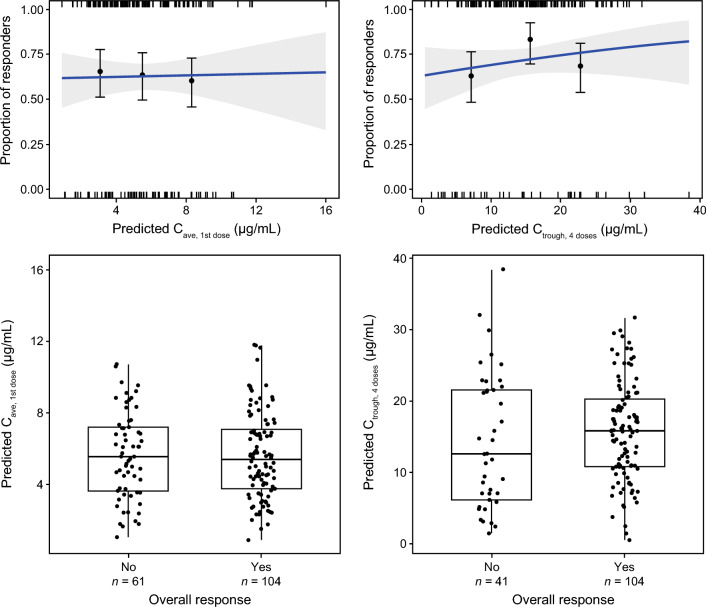
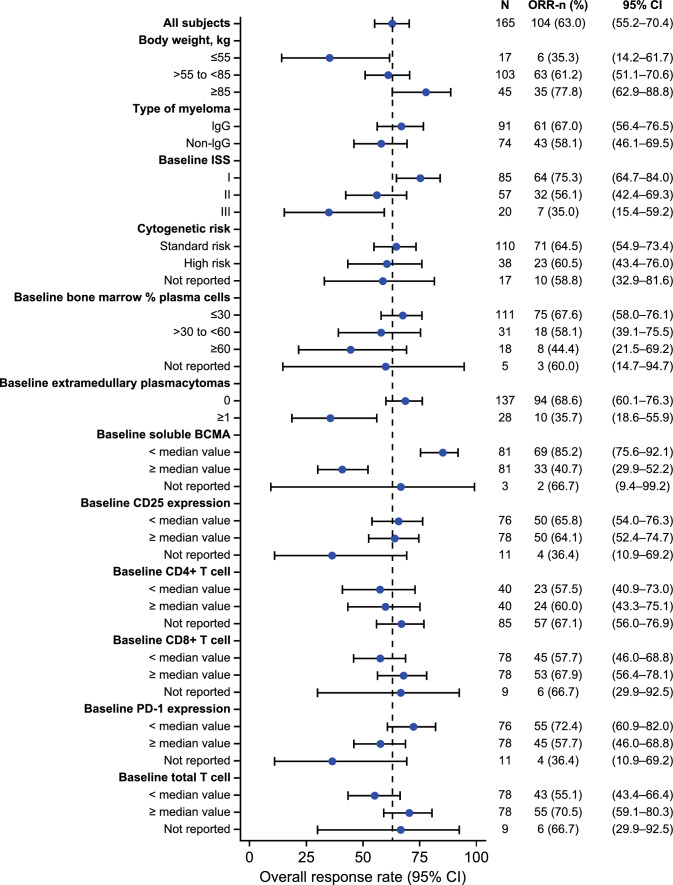
Results: In total, 4840 measurable serum concentration samples from 338 pharmacokinetics-evaluable patients who received teclistamab were analyzed. The typical population value of time-independent and time-dependent clearance were 0.449 L/day and 0.547 L/day, respectively. The time-dependent clearance decreased rapidly to < 10% after 8 weeks of teclistamab treatment. Patients who discontinue teclistamab after the 13th dose are expected to have a 50% reduction from Cmax in teclistamab concentration at a median (5th to 95th percentile) time of 15 days (7-33 days) after Tmax and a 97% reduction from Cmax in teclistamab concentration at a median time of 69 days (32-163 days) after Tmax. Body weight, multiple myeloma type (immunoglobulin G vs non-immunoglobulin G), and International Staging System (ISS) stage (II vs I and III vs I) were statistically significant covariates on teclistamab pharmacokinetics; however, these covariates had no clinically relevant effect on the efficacy of teclistamab at the RP2D. Across all doses, ORR approached a plateau at the concentration range associated with RP2D, and in patients who received the RP2D, a flat exposure-response curve was observed. No apparent relationship was observed between DoR, PFS, OS, and the incidence of grade ≥3 adverse events across the predicted exposure quartiles.
Conclusion: Body weight, myeloma type, and ISS stage impacted systemic teclistamab exposure without any clinically relevant effect on efficacy. The exposure-response analyses for ORR showed a positive trend with increasing teclistamab systemic exposure, with a plateau at the RP2D, and there was no apparent exposure-response trend for safety or other efficacy endpoints. These analyses support the RP2D of teclistamab in patients with RRMM.
Clinical trial registration: NCT03145181 (phase I, 09 May 2017); NCT04557098 (phase II, 21 September 2020).
© 2023. The Author(s).
Conflict of interest statement
Xin Miao, Liviawati S. Wu, Yuki Iwaki, Rachel Kobos, Tara Stephenson, Kristy Kemmerer, Clarissa M. Uhlar, Arnob Banerjee, Danielle Trancucci, Amit Apte, Raluca Verona, Lixia Pei, Rachit Desai, Kathleen Hickey, Yaming Su, Daniele Ouellet, Mahesh Samtani, and Yue Guo are employees of Janssen. Shun Xin Wang Lin is an employee of LinkiDose Medicine Co., Ltd. Yan Xu is an employee of Simcere Pharmaceuticals. Yang Chen is an employee of Daiichi Sankyo. Jenna D. Goldberg is an employee of Vividon and holds stock in Janssen. Alfred L. Garfall is a consultant for Janssen, GSK, and Amgen; has received research funding from Janssen, Novartis, Tmunity, and CRISPR Therapeutics; and is an independent data monitoring committee member for Janssen. Amrita Krishnan is a consultant for Adaptive, Janssen, Sanofi, BMS, Pfizer, and Regneron; is a current equity holder in BMS; has received research funding from Janssen; is a Speakers’ Bureau member for Takeda, GSK, and BMS; and is a member of the Board of Directors or advisory committee for Sutro. Saad Z. Usmani has served in a consulting or advisory role for Celgene, Amgen, Janssen, Takeda, GlaxoSmithKline, Karyopharm Therapeutics, AbbVie, Merck, Genentech, Gilead Sciences, and Bristol-Myers Squibb/Celgene; and has received research funding from Celgene, Array BioPharma, Janssen, Pharmacyclics, Sanofi, Bristol-Myers Squibb, Amgen, Seattle Genetics, Merck, Skyline Diagnostics, and GlaxoSmithKline. Honghui Zhou is an employee of Jazz Pharmaceuticals and owns stocks in Jazz Pharmaceuticals and Johnson & Johnson. Suzette Girgis is an employee of Jazz Pharmaceuticals and holds stocks in JNJ and BMS.
Figures
References
-
- EMA summary of product characteristics. Abecma (idecabtagene vicleucel). Vol. 2022.
-
- EMA summary of product characteristics. CARVYKTI (ciltacabtagene autoleucel). Vol. 2022.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
