

The HERA (Hyper-response Risk Assessment) Delphi consensus for the management of hyper-responders in in vitro fertilization
- PMID: 37713144
- PMCID: PMC10643792
- DOI: 10.1007/s10815-023-02918-5
The HERA (Hyper-response Risk Assessment) Delphi consensus for the management of hyper-responders in in vitro fertilization
Erratum in
-
Correction to: The HERA (Hyper‑response Risk Assessment) Delphi consensus for the management of hyper‑responders in in vitro fertilization.J Assist Reprod Genet. 2024 Feb;41(2):519-520. doi: 10.1007/s10815-023-03003-7. J Assist Reprod Genet. 2024. PMID: 38079078 Free PMC article. No abstract available.
Abstract
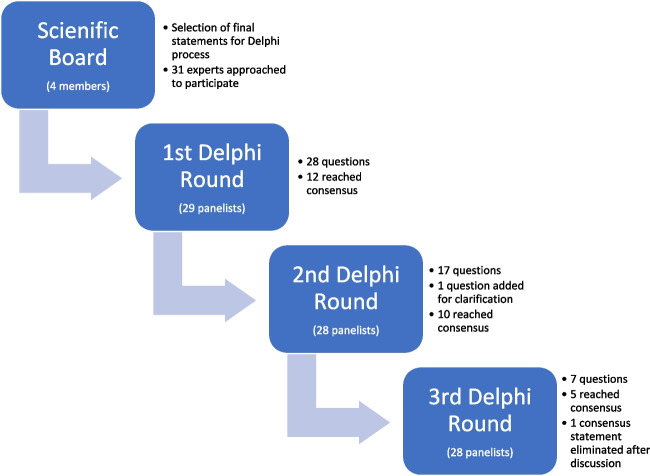
Purpose: To provide agreed-upon guidelines on the management of a hyper-responsive patient undergoing ovarian stimulation (OS) METHODS: A literature search was performed regarding the management of hyper-response to OS for assisted reproductive technology. A scientific committee consisting of 4 experts discussed, amended, and selected the final statements. A priori, it was decided that consensus would be reached when ≥66% of the participants agreed, and ≤3 rounds would be used to obtain this consensus. A total of 28/31 experts responded (selected for global coverage), anonymous to each other.
Results: A total of 26/28 statements reached consensus. The most relevant are summarized here. The target number of oocytes to be collected in a stimulation cycle for IVF in an anticipated hyper-responder is 15-19 (89.3% consensus). For a potential hyper-responder, it is preferable to achieve a hyper-response and freeze all than aim for a fresh transfer (71.4% consensus). GnRH agonists should be avoided for pituitary suppression in anticipated hyper-responders performing IVF (96.4% consensus). The preferred starting dose in the first IVF stimulation cycle of an anticipated hyper-responder of average weight is 150 IU/day (82.1% consensus). ICoasting in order to decrease the risk of OHSS should not be used (89.7% consensus). Metformin should be added before/during ovarian stimulation to anticipated hyper-responders only if the patient has PCOS and is insulin resistant (82.1% consensus). In the case of a hyper-response, a dopaminergic agent should be used only if hCG will be used as a trigger (including dual/double trigger) with or without a fresh transfer (67.9% consensus). After using a GnRH agonist trigger due to a perceived risk of OHSS, luteal phase rescue with hCG and an attempt of a fresh transfer is discouraged regardless of the number of oocytes collected (72.4% consensus). The choice of the FET protocol is not influenced by the fact that the patient is a hyper-responder (82.8% consensus). In the cases of freeze all due to OHSS risk, a FET cycle can be performed in the immediate first menstrual cycle (92.9% consensus).
Conclusion: These guidelines for the management of hyper-response can be useful for tailoring patient care and for harmonizing future research.
Keywords: Hyper-response; Ovarian hyperstimulation syndrome; Ovarian stimulation.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
All declarations of interest are outside the submitted work. Peter Humaidan reports reception of lecture honoraria from Merck, Gedeon Richter, and IBSA. Antonio La Marca reports reception of consulting fees from Merck, Organon, Ferring, Gedeon Richter, Theramex, Beckman Coulter, and Roche. Samuel Santos-Ribeiro reports reception of research funding from Roche Diagnostics, Organon, and Theramex; reception of consulting fees from Organon, MSD, and Ferring; honoraria for lectures from Ferring, Besins, MSD/Organon, Theramex, and Gedeon Richter; reception of equipment materials or other services from Roche Diagnostics and Ferring; and is deputy of the SQART SIG in ESHRE. Alessandro Conforti reports reception of grants from the University of Naples Federico II; reception honoraria from Medea, Event Planet, and Merck. Baris Ata reports reception of consulting fees from Merck GmBH–Turkey; reception of payment or honoraria from Abbott, Merck GmBH, and Ferring; reception of support for attending meetings or travel from IBSA; is president of the Turkish Society of Reproductive Medicine; and is an executive committee member of ESHRE. Juan Garcia Velasco reports reception of payment or honoraria for lectures or educational events from Merck, Ferring, MSD, Organon, Theramex, and Gedeon Richter. George Lainas reports reception of payment or honoraria for lectures or educational events from Merck and Ferring, payment for expert testimony from Merck, and support for attending meetings from ESHRE. He also participated in data safety monitoring or advisory board of Merck. Filippo Maria Ubaldi is the scientific director of GeneraLife and minority shareholder of the company. He is also the president of SIFES-MR (the Italian Society of Fertility, Sterility and Reproductive Medicine) and a member of the scientific board of Medea. In the last 3 years, F.M. Ubaldi has received honoraria or consultation fees from Merck, MSD, Ferring, Gedeon Richter, Organon, and IBSA. Sesh Sunkara reports reception of payment or honoraria for lectures from Merck Ferring and MSD. Raoul Orvieto reports reception of consulting fees from Merck and Ferring and payment or honoraria for lectures from Merck and Ferring. Nikolaos Polyzos reports reception of grants or contracts from Merck Serono, IBSA, Organon, Ferring, Roche, Theramex, Besins Healthcare, and Gedeon Richter and reception of consulting fees from Merck Serono, IBSA, Organon, Ferring, Besins Healthcare, and Gedeon Richter. Hakan Yarali reports unrestricted grants from Merck, honoraria for lectures from Merck and IBSA, and support for attending meetings from Merck, IBSA, and Ferring. Human Fatemi reports receiving research grants from Merck Serono and Organon; consulting fees from Ferring Global; speaker honoraria from Organon, Merck Serono, and Ferring; and participation in data safety monitoring or advisory board for Ferring. Sandro Esteves reports unrestricted research grants from Merck KGaA; reception of consulting fees from Merck, MeD.E.A, and event planet; reception of honoraria for lectures from Merck, MeD.E.A, and event planet; has a patent on the ART calculator, is an unpaid advisory board member for Nature Reviews and for Urology, Is the Head, Department of Education and Research, Brazilian Society of Urology (São Paulo section; unpaid), and is the Co-chair, Male Infertility Special Interest Group, WHO Infertility Guidelines (unpaid). Craig LaTasha is a site investigator for Ferring Pharmaceuticals. He was an advisory board member for Ferring Pharmaceuticals. Ariel Weissman, Christophe Blockeel, Christos Venetis, Seang Lin Tan, Michael Dahan, Bulent Urman, RJ Norman, Richard Paulson, and Ido Feferkorn report no conflicts of interest.
References
-
- Polyzos NP, Drakopoulos P, Parra J, Pellicer A, Santos-Ribeiro S, Tournaye H, et al. Cumulative live birth rates according to the number of oocytes retrieved after the first ovarian stimulation for in vitro fertilization/intracytoplasmic sperm injection: a multicenter multinational analysis including ∼15,000 women. Fertil Steril [Internet]. 2018;110:661–670.e1. doi: 10.1016/j.fertnstert.2018.04.039. - DOI - PubMed
-
- Bosdou JK, Venetis CA, Tarlatzis BC, Grimbizis GF, Kolibianakis EM. Higher probability of live-birth in high, but not normal, responders after first frozen-embryo transfer in a freeze-only cycle strategy compared to fresh-embryo transfer: a meta-analysis. Hum Reprod [Internet]. 2019;34:491–505. doi: 10.1093/humrep/dey388. - DOI - PubMed
-
- Boynukalin FK, Turgut NE, Gultomruk M, Ecemis S, Yarkiner Z, Findikli N, et al. Impact of elective frozen vs. fresh embryo transfer strategies on cumulative live birth: Do deleterious effects still exist in normal & hyper responders? PLoS One. 2020;15 [cited 2022 Mar 17]; Available from: https://pubmed-ncbi-nlm-nih-gov.proxy3.library.mcgill.ca/32589634/ - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
