

Medicare Advantage Enrollment and Disenrollment Among Persons With Alzheimer Disease and Related Dementias
- PMID: 37713210
- PMCID: PMC10504614
- DOI: 10.1001/jamahealthforum.2023.3080
Medicare Advantage Enrollment and Disenrollment Among Persons With Alzheimer Disease and Related Dementias
Abstract
Importance: Large enrollment growth has been observed in the Medicare Advantage program, but less is known about enrollment patterns among persons with Alzheimer disease and related dementias (ADRD).
Objective: To evaluate patterns in Medicare Advantage enrollment and disenrollment among beneficiaries with or without ADRD.
Design, setting, and participants: This cross-sectional study used 6 national data sources between January 1, 2011, and December 31, 2018. Analyses were performed between June 2021 and August 2022. The cohort comprised US Medicare beneficiaries with acute or postacute care utilization between 2013 and 2018.
Exposure: ADRD diagnosis from an acute or postacute care encounter Medicare data source.
Main outcomes and measures: Enrollment in Medicare Advantage, disenrollment from Medicare Advantage to traditional Medicare, and contract exit (leaving a Medicare Advantage contract for traditional Medicare or a different Medicare Advantage contract).
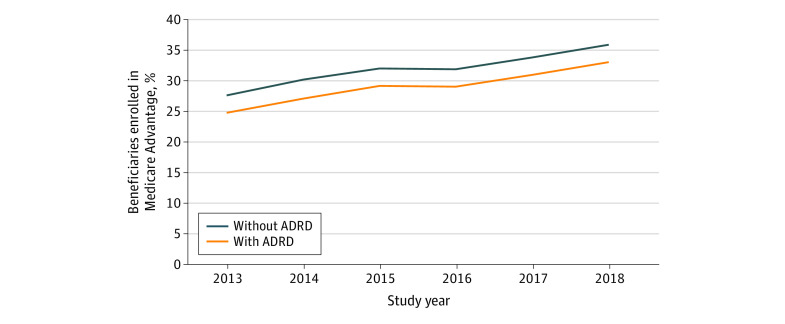
Results: The 32 796 872 Medicare beneficiaries in the cohort had a mean (SD) age of 74.0 (12.5) years and included 18 228 513 females (55.6%). Enrollment in Medicare Advantage among beneficiaries with ADRD increased from 24.7% (95% CI, 24.7%-24.8%) in 2013 to 33.0% (95% CI, 32.9%-33.1%) in 2018, an absolute increase of 8.3 percentage points and a 33.4% relative increase after adjusting for demographic characteristics, comorbid conditions, and utilization and including county fixed effects. Among beneficiaries without ADRD, enrollment in Medicare Advantage increased by 8.2 percentage points from 27.6% (95% CI, 27.6%-27.6%) in 2013 to 35.8% (95% CI, 35.8%-35.8%) in 2018, a 29.7% relative increase over the study period. Beneficiaries with ADRD were 1.4 times as likely to disenroll from their Medicare Advantage contract to traditional Medicare (4.4% vs 3.2% in 2017-2018; P < .001) in adjusted analyses. Regardless of ADRD status, beneficiaries had similar rates of switching to a new Medicare Advantage contract. Differences in contract exit rates were associated with higher rates of disenrollment from Medicare Advantage to traditional Medicare among beneficiaries with ADRD vs those without ADRD (16.3% [95% CI, 16.2%-16.3%] vs 15.1% [95% CI, 15.1%-15.1%]). Beneficiaries with ADRD and dual eligibility for Medicaid enrollment had higher rates of contract exit than those without dual eligibility (19.7% [95% CI, 19.6%-19.7%] vs 14.9% [95% CI, 14.8%-14.9%]), and these differences were even greater than those among beneficiaries without ADRD and with and without dual-eligibility status, respectively (18.3% [95% CI, 18.2%-18.3%] vs 13.8% [95% CI, 13.7%-13.8%]).
Conclusions and relevance: In this cross-sectional study of the Medicare population with acute and postacute care use, beneficiaries with ADRD had increasing enrollment in the Medicare Advantage program, proportional to the growth in overall enrollment, but their disenrollment from Medicare Advantage in the following year remained higher compared with beneficiaries without ADRD. The findings highlight the need to understand the factors associated with higher disenrollment rates and determine whether such rates reflect access or quality challenges for beneficiaries with ADRD.
Conflict of interest statement
Figures


Similar articles
-
Outcomes for Dual-Eligible Beneficiaries With Dementia in Special Needs Plans and Other Medicare Advantage Plans.JAMA Netw Open. 2025 Feb 3;8(2):e2461219. doi: 10.1001/jamanetworkopen.2024.61219. JAMA Netw Open. 2025. PMID: 39982721 Free PMC article.
-
Analysis of Drivers of Disenrollment and Plan Switching Among Medicare Advantage Beneficiaries.JAMA Intern Med. 2019 Apr 1;179(4):524-532. doi: 10.1001/jamainternmed.2018.7639. JAMA Intern Med. 2019. PMID: 30801625 Free PMC article.
-
Health Care Utilization, Care Satisfaction, and Health Status for Medicare Advantage and Traditional Medicare Beneficiaries With and Without Alzheimer Disease and Related Dementias.JAMA Netw Open. 2020 Mar 2;3(3):e201809. doi: 10.1001/jamanetworkopen.2020.1809. JAMA Netw Open. 2020. PMID: 32227181 Free PMC article.
-
Case Definition for Diagnosed Alzheimer Disease and Related Dementias in Medicare.JAMA Netw Open. 2024 Sep 3;7(9):e2427610. doi: 10.1001/jamanetworkopen.2024.27610. JAMA Netw Open. 2024. PMID: 39226058 Free PMC article.
-
Impact of star ratings on Medicare health plan enrollment: A systematic literature review.J Am Pharm Assoc (2003). 2023 Jul-Aug;63(4):989-997.e3. doi: 10.1016/j.japh.2023.03.009. Epub 2023 Apr 3. J Am Pharm Assoc (2003). 2023. PMID: 37019381
Cited by
-
Trends in Co-morbid Dementia and Chronic Kidney Disease.J Gen Intern Med. 2025 Jul;40(10):2276-2283. doi: 10.1007/s11606-024-09069-y. Epub 2025 Jan 14. J Gen Intern Med. 2025. PMID: 39809960
-
Disenrollment From Special Needs and Other Medicare Advantage Plans Among Nursing Home Residents.JAMA Netw Open. 2025 Jul 1;8(7):e2523973. doi: 10.1001/jamanetworkopen.2025.23973. JAMA Netw Open. 2025. PMID: 40742596 Free PMC article.
-
Medicare Advantage enrollment and outcomes of post-acute nursing home care among patients with dementia.Health Aff Sch. 2024 Jun 13;2(6):qxae084. doi: 10.1093/haschl/qxae084. eCollection 2024 Jun. Health Aff Sch. 2024. PMID: 38934015 Free PMC article.
-
The effect of providing Medicare Advantage enrollees diagnosed with cancer additional time to reassess enrollment.Health Aff Sch. 2025 Jun 27;3(7):qxaf131. doi: 10.1093/haschl/qxaf131. eCollection 2025 Jul. Health Aff Sch. 2025. PMID: 40657590 Free PMC article.
-
Differences in setting of initial dementia diagnosis among fee-for-service Medicare beneficiaries.J Am Geriatr Soc. 2025 Jan;73(1):39-49. doi: 10.1111/jgs.19236. Epub 2024 Oct 22. J Am Geriatr Soc. 2025. PMID: 39434608
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
