

Adverse childhood experiences: a meta-analysis of prevalence and moderators among half a million adults in 206 studies
- PMID: 37713544
- PMCID: PMC10503911
- DOI: 10.1002/wps.21122
Adverse childhood experiences: a meta-analysis of prevalence and moderators among half a million adults in 206 studies
Abstract
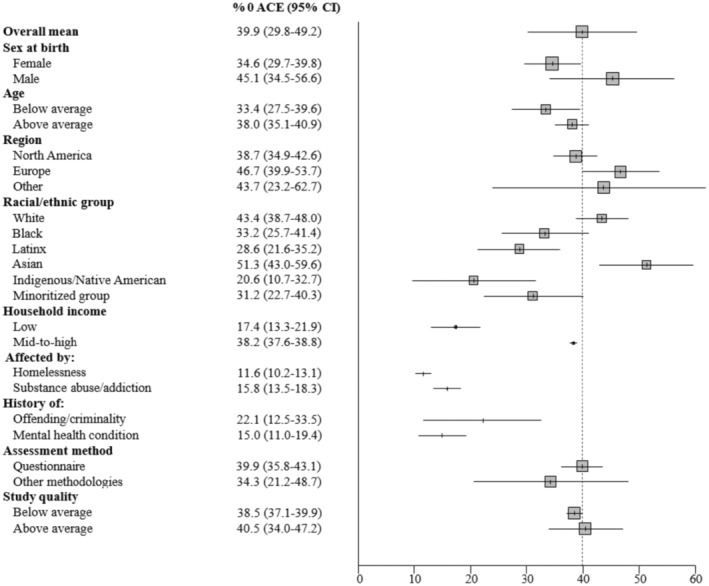
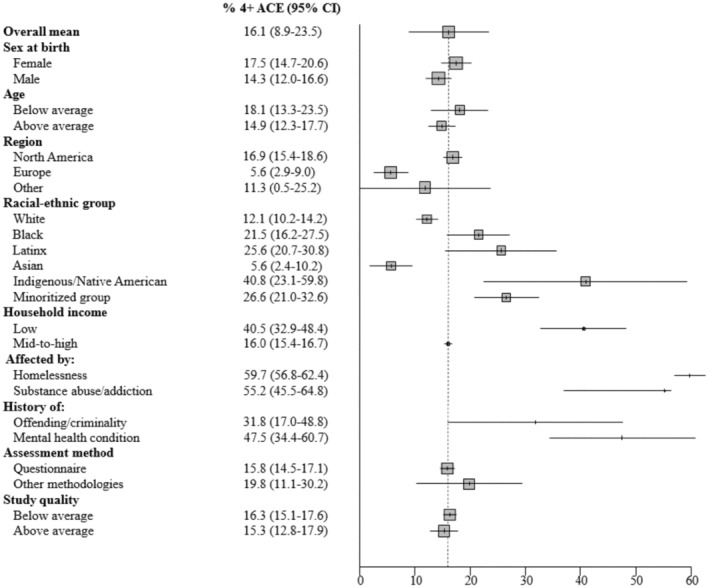
Exposure to adverse childhood experiences (ACEs), including maltreatment and family dysfunction, is a major contributor to the global burden of disease and disability. With a large body of international literature on ACEs having emerged over the past 25 years, it is timely to now synthetize the available evidence to estimate the global prevalence of ACEs and, through a series of moderator analyses, determine which populations are at higher risk. We searched studies published between January 1, 1998 and August 5, 2021 in Medline, PsycINFO and Embase. Study inclusion criteria were using the 8- or 10-item ACE Questionnaire (±2 items), reporting the prevalence of ACEs in population samples of adults, and being published in English. The review protocol was registered with PROSPERO (CRD42022348429). In total, 206 studies (208 sample estimates) from 22 countries, with 546,458 adult participants, were included. The pooled prevalence of the five levels of ACEs was: 39.9% (95% CI: 29.8-49.2) for no ACE; 22.4% (95% CI: 14.1-30.6) for one ACE; 13.0% (95% CI: 6.5-19.8) for two ACEs; 8.7% (95% CI: 3.4-14.5) for three ACEs, and 16.1% (95% CI: 8.9-23.5) for four or more ACEs. In subsequent moderation analyses, there was strong evidence that the prevalence of 4+ ACEs was higher in populations with a history of a mental health condition (47.5%; 95% CI: 34.4-60.7) and with substance abuse or addiction (55.2%; 95% CI: 45.5-64.8), as well as in individuals from low-income households (40.5%; 95% CI: 32.9-48.4) and unhoused individuals (59.7%; 95% CI: 56.8-62.4). There was also good evidence that the prevalence of 4+ ACEs was larger in minoritized racial/ethnic groups, particularly when comparing study estimates in populations identifying as Indigenous/Native American (40.8%; 95% CI: 23.1-59.8) to those identifying as White (12.1%; 95% CI: 10.2-14.2) and Asian (5.6%; 95% CI: 2.4-10.2). Thus, ACEs are common in the general population, but there are disparities in their prevalence. They are among the principal antecedent threats to individual well-being and, as such, constitute a pressing social issue globally. Both prevention strategies and downstream interventions are needed to reduce the prevalence and mitigate the severity of the effects of ACEs and thereby reduce their deleterious health consequences on future generations.
Keywords: Adverse childhood experiences; low-income households; mental health conditions; racial/ethnic minorities; substance abuse; unhoused individuals.
© 2023 World Psychiatric Association.
Figures

References
-
- Felitti VJ, Anda RF, Nordenberg D. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) study. Am J Prev Med 1998;14:245‐58. - PubMed
-
- Hughes K, Bellis MA, Hardcastle KA et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta‐analysis. Lancet Public Health 2017;2:e356‐66. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
