

Comorbidity between major depressive disorder and physical diseases: a comprehensive review of epidemiology, mechanisms and management
- PMID: 37713568
- PMCID: PMC10503929
- DOI: 10.1002/wps.21110
Comorbidity between major depressive disorder and physical diseases: a comprehensive review of epidemiology, mechanisms and management
Abstract
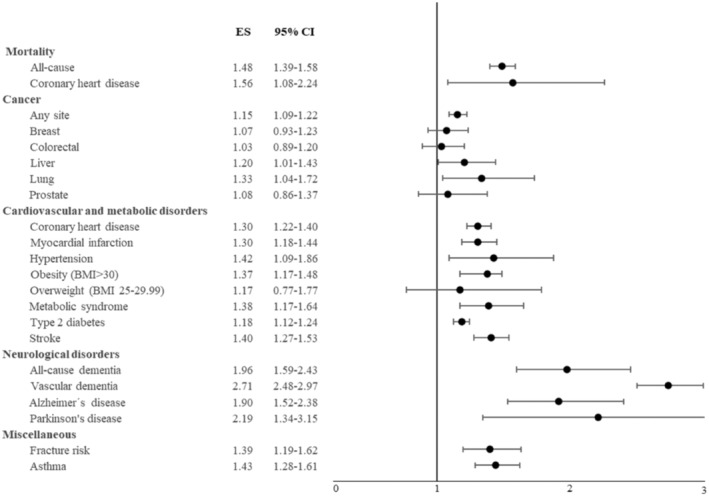
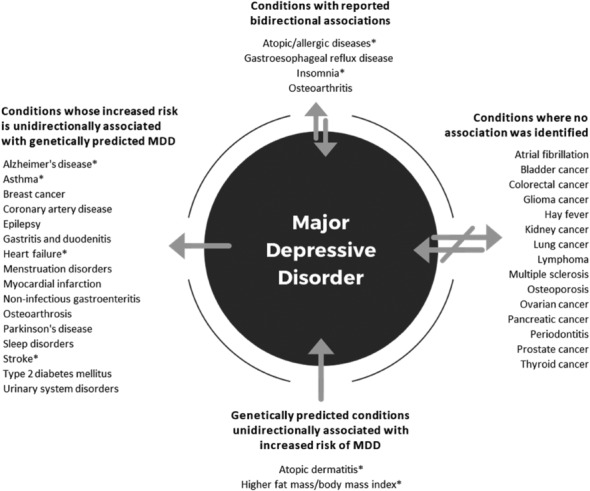
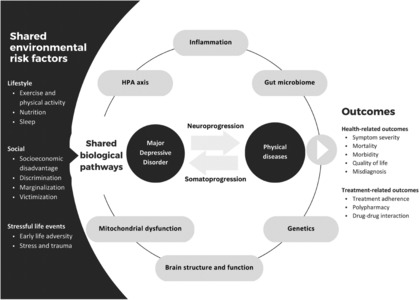
Populations with common physical diseases - such as cardiovascular diseases, cancer and neurodegenerative disorders - experience substantially higher rates of major depressive disorder (MDD) than the general population. On the other hand, people living with MDD have a greater risk for many physical diseases. This high level of comorbidity is associated with worse outcomes, reduced adherence to treatment, increased mortality, and greater health care utilization and costs. Comorbidity can also result in a range of clinical challenges, such as a more complicated therapeutic alliance, issues pertaining to adaptive health behaviors, drug-drug interactions and adverse events induced by medications used for physical and mental disorders. Potential explanations for the high prevalence of the above comorbidity involve shared genetic and biological pathways. These latter include inflammation, the gut microbiome, mitochondrial function and energy metabolism, hypothalamic-pituitary-adrenal axis dysregulation, and brain structure and function. Furthermore, MDD and physical diseases have in common several antecedents related to social factors (e.g., socioeconomic status), lifestyle variables (e.g., physical activity, diet, sleep), and stressful live events (e.g., childhood trauma). Pharmacotherapies and psychotherapies are effective treatments for comorbid MDD, and the introduction of lifestyle interventions as well as collaborative care models and digital technologies provide promising strategies for improving management. This paper aims to provide a detailed overview of the epidemiology of the comorbidity of MDD and specific physical diseases, including prevalence and bidirectional risk; of shared biological pathways potentially implicated in the pathogenesis of MDD and common physical diseases; of socio-environmental factors that serve as both shared risk and protective factors; and of management of MDD and physical diseases, including prevention and treatment. We conclude with future directions and emerging research related to optimal care of people with comorbid MDD and physical diseases.
Keywords: Depression; cancer; cardiovascular diseases; childhood trauma; collaborative care; comorbidity; digital technologies; inflammation; lifestyle factors; physical diseases.
© 2023 World Psychiatric Association.
Figures

References
-
- Ferrari A, Somerville A, Baxter A et al. Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med 2013;43:471‐81. - PubMed
-
- Scott AJ, Sharpe L, Hunt C et al. Anxiety and depressive disorders in people with epilepsy: a meta‐analysis. Epilepsia 2017;58:973‐82. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
