

Optimal cutoff point of vertebral body cross-sectional area as a morphological parameter for predicting lumbar spondylolysis
- PMID: 37713872
- PMCID: PMC10508529
- DOI: 10.1097/MD.0000000000035173
Optimal cutoff point of vertebral body cross-sectional area as a morphological parameter for predicting lumbar spondylolysis
Abstract
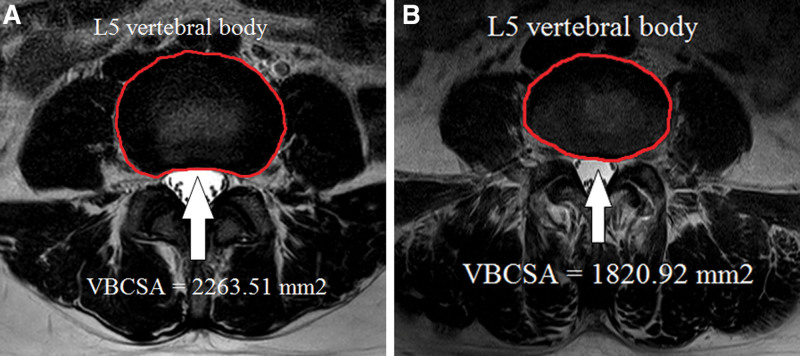
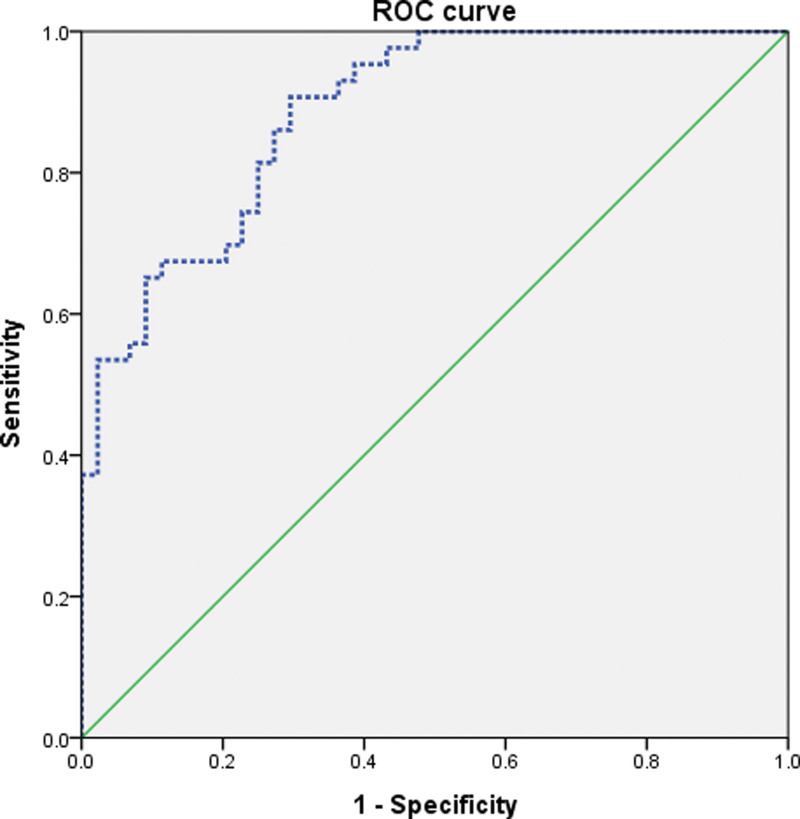
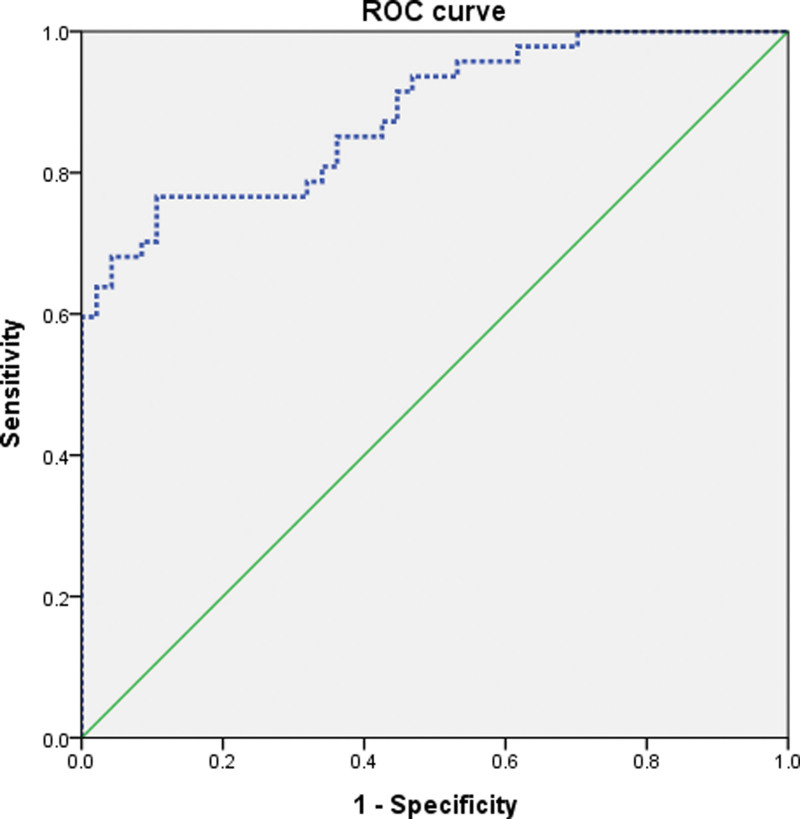
The relationship between vertebral body cross-sectional area (VBCSA) and spinal conditions associated with increased lumbar lordosis, such as lumbar spondylolysis (LSL), is not known. We investigated the morphological parameter, VBCSA, to predict LSL. The VBCSA on MRI has not been studied for its association with LSL. We hypothesized that VBCSA is an important morphological parameter for LSL prediction. We collected VBCSA data from 90 patients (43 males and 47 females) with LSL and 91 control subjects (44 males and 47 females) who underwent lumbar spine magnetic resonance imaging (LS-MRI). Axial T2-weighted LS-MRI images were obtained from all participants. Using our picture archiving and communications system, we analyzed the VBCSA at the level of the L5 vertebral body by utilizing MRI. The average VBCSA was 2263.51 ± 306.02 mm2 in the male control group and 1820.92 ± 224.89 mm2 in the male LSL group. LSL patients had significantly lower VBCSAs (P < .001) than did the male controls. The average VBCSA was 1985.21 ± 258.05 mm2 in the female control group and 1553.73 ± 250.02 mm2 in the female LSL group, and the LSL patients also had significantly lower VBCSAs (P < .001) than did the female controls. The optimal VBCSA cutoff value in the male group was 2014.69 mm2 with 76.7% sensitivity, 75.0% specificity, and an area under the receiver operating curve (AUC) of 0.89 (95% CI: 0.82-0.95). In the female group, the optimal cutoff score was 1814.11 mm2 with 76.6% sensitivity, 76.6% specificity, and an AUC of 0.88 (95% CI: 0.82-0.95). VBCSA is a sensitive objective morphological parameter for assessing LSL, and a lower VBCSA is associated with a higher possibility of LSL. We believe that these results will be useful in diagnostic radiology for evaluating patients with LSL.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Increased Lumbar Lordosis and Smaller Vertebral Cross-Sectional Area Are Associated With Spondylolysis.Spine (Phila Pa 1976). 2018 Jun 15;43(12):833-838. doi: 10.1097/BRS.0000000000002480. Spine (Phila Pa 1976). 2018. PMID: 29095410
-
The Role of the Ligamentum Flavum Area as a Morphological Parameter of Lumbar Central Spinal Stenosis.Pain Physician. 2017 Mar;20(3):E419-E424. Pain Physician. 2017. PMID: 28339441
-
Significance of interfacet distance, facet joint orientation, and lumbar lordosis in spondylolysis.Clin Anat. 2012 Apr;25(3):391-7. doi: 10.1002/ca.21222. Epub 2011 Aug 3. Clin Anat. 2012. PMID: 21815218
-
Dural sac area is a more sensitive parameter for evaluating lumbar spinal stenosis than spinal canal area: A retrospective study.Medicine (Baltimore). 2017 Dec;96(49):e9087. doi: 10.1097/MD.0000000000009087. Medicine (Baltimore). 2017. PMID: 29245329 Free PMC article.
-
Double-level lumbar spondylolysis and spondylolisthesis: A retrospective study.J Orthop Surg Res. 2018 Mar 16;13(1):55. doi: 10.1186/s13018-018-0723-3. J Orthop Surg Res. 2018. PMID: 29548343 Free PMC article. Review.
Cited by
-
Comparative analysis of morphologival parameters in isolated and fused L5 spondylolysis patients on the basis of CT features.BMC Musculoskelet Disord. 2025 Feb 1;26(1):104. doi: 10.1186/s12891-025-08357-w. BMC Musculoskelet Disord. 2025. PMID: 39893376 Free PMC article.
References
-
- Wren TAL, Ponrartana S, Aggabao PC, et al. . Increased lumbar lordosis and smaller vertebral cross-sectional area are associated with spondylolysis. Spine (Phila Pa 1976). 2018;43:833–8. - PubMed
-
- Donnally IC, Varacallo M. Lumbar Spondylolysis and Spondylolisthesis. Treasure Island, FL: StatPearls; 2018. - PubMed
-
- Iwaki K, Sakai T, Hatayama D, et al. . Physical features of pediatric patients with lumbar spondylolysis and effectiveness of rehabilitation. J Med Invest. 2018;65:177–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
