

Electronic Health Records (EHRs) Can Identify Patients at High Risk of Fracture but Require Substantial Race Adjustments to Currently Available Fracture Risk Calculators
- PMID: 37715097
- PMCID: PMC10713897
- DOI: 10.1007/s11606-023-08347-5
Electronic Health Records (EHRs) Can Identify Patients at High Risk of Fracture but Require Substantial Race Adjustments to Currently Available Fracture Risk Calculators
Abstract
Background: Osteoporotic fracture prediction calculators are poorly utilized in primary care, leading to underdiagnosis and undertreatment of those at risk for fracture. The use of these calculators could be improved if predictions were automated using the electronic health record (EHR). However, this approach is not well validated in multi-ethnic populations, and it is not clear if the adjustments for race or ethnicity made by calculators are appropriate.
Objective: To investigate EHR-generated fracture predictions in a multi-ethnic population.
Design: Retrospective cohort study using data from the EHR.
Setting: An urban, academic medical center in Philadelphia, PA.
Participants: 12,758 White, 7,844 Black, and 3,587 Hispanic patients seeking routine care from 2010 to 2018 with mean 3.8 years follow-up.
Interventions: None.
Measurements: FRAX and QFracture, two of the most used fracture prediction tools, were studied. Risk for major osteoporotic fracture (MOF) and hip fracture were calculated using data from the EHR at baseline and compared to the number of fractures that occurred during follow-up.
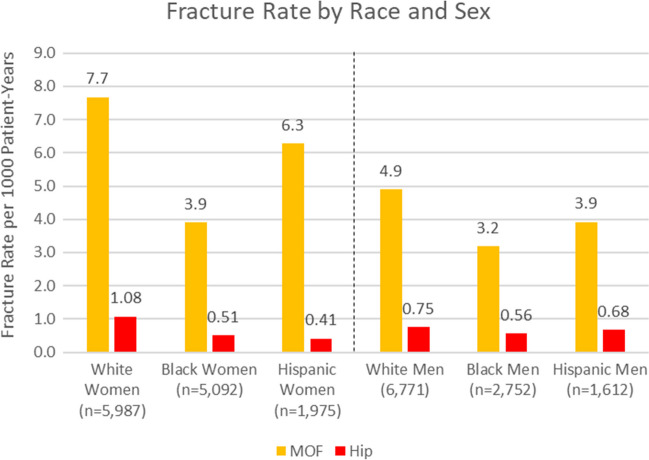
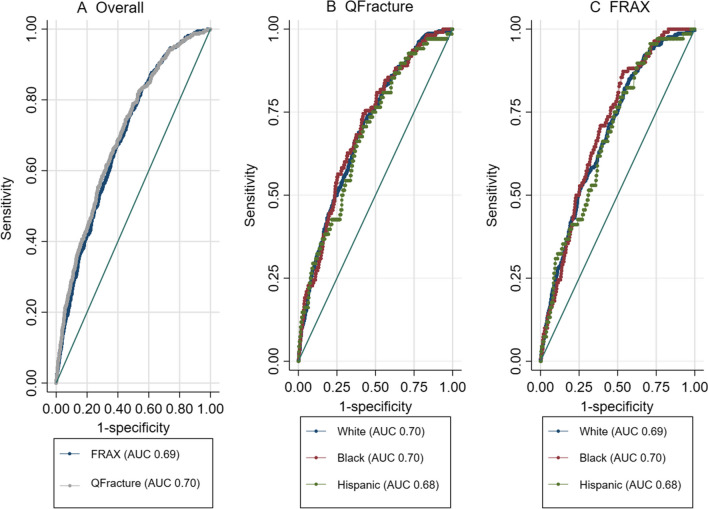
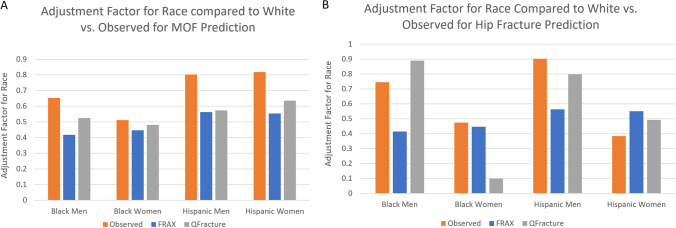
Results: MOF rates varied from 3.2 per 1000 patient-years in Black men to 7.6 in White women. FRAX and QFracture had similar discrimination for MOF prediction (area under the curve, AUC, 0.69 vs. 0.70, p=0.08) and for hip fracture prediction (AUC 0.77 vs 0.79, p=0.21) and were similar by race or ethnicity. FRAX had superior calibration than QFracture (calibration-in-the-large for FRAX 0.97 versus QFracture 2.02). The adjustment factors used in MOF prediction were generally accurate in Black women, but underestimated risk in Black men, Hispanic women, and Hispanic men.
Limitations: Single center design.
Conclusions: Fracture predictions using only EHR inputs can discriminate between high and low risk patients, even in Black and Hispanic patients, and could help primary care physicians identify patients who need screening or treatment. However, further refinements to the calculators may better adjust for race-ethnicity.
Keywords: black; electronic medical record; ethnicity; fracture; hispanic; osteoporosis; race.
© 2023. The Author(s), under exclusive licence to Society of General Internal Medicine.
Figures
References
-
- Siu A, Allore H, Brown D, Charles ST, Lohman M. National Institutes of Health Pathways to Prevention Workshop: Research Gaps for Long-Term Drug Therapies for Osteoporotic Fracture Prevention. Ann Intern Med. 2019;171:51–57. - PubMed
-
- Bone Health & Osteoporosis Foundation [Internet]. [cited 2023 Apr 18]. General Facts. Available from: https://www.bonehealthandosteoporosis.org/preventing-fractures/general-f.... Accessed 18 Apr 2023
-
- Desai RJ, Mahesri M, Abdia Y, Barberio J, Tong A, Zhang D, et al. Association of osteoporosis medication use after hip fracture with prevention of subsequent nonvertebral fractures: an instrumental variable analysis. JAMA Netw Open. 2018;1(3):e180826–e180826. doi: 10.1001/jamanetworkopen.2018.0826. - DOI - PMC - PubMed
-
- Beaudoin C, Moore L, Gagné M, Bessette L, Ste-Marie LG, Brown JP, et al. Performance of predictive tools to identify individuals at risk of non-traumatic fracture: a systematic review, meta-analysis, and meta-regression. Osteoporos Int. 2019;30:721–740. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
