

Reversible cardiac function and left ventricular hypertrophy in a Chinese man with mitochondrial myopathy: a case report
- PMID: 37715114
- PMCID: PMC10503081
- DOI: 10.1186/s12872-023-03444-z
Reversible cardiac function and left ventricular hypertrophy in a Chinese man with mitochondrial myopathy: a case report
Abstract
Background: Mitochondrial myopathies (MMs) are a group of multi-system diseases caused by abnormalities in mitochondrial DNA (mtDNA) or mutations of nuclear DNA (nDNA). The diagnosis of mitochondrial myopathy (MM) is reliant on the combination of history and physical examination, muscle biopsy, histochemical studies, and next-generation sequencing. Patients with MMs have diverse clinical manifestations. In the contemporary literature, there is a paucity of reports on cardiac structure and function in this rare disease. We report a Chinese man with MM accompanied with both acute right heart failure and left ventricular hypertrophy.
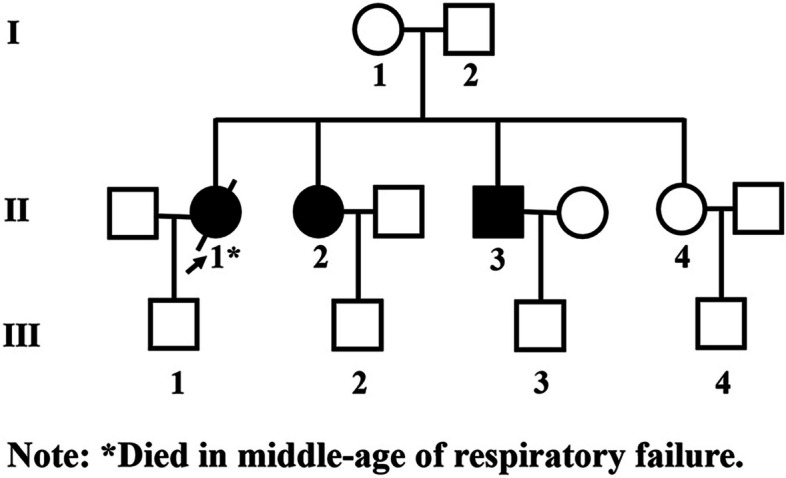
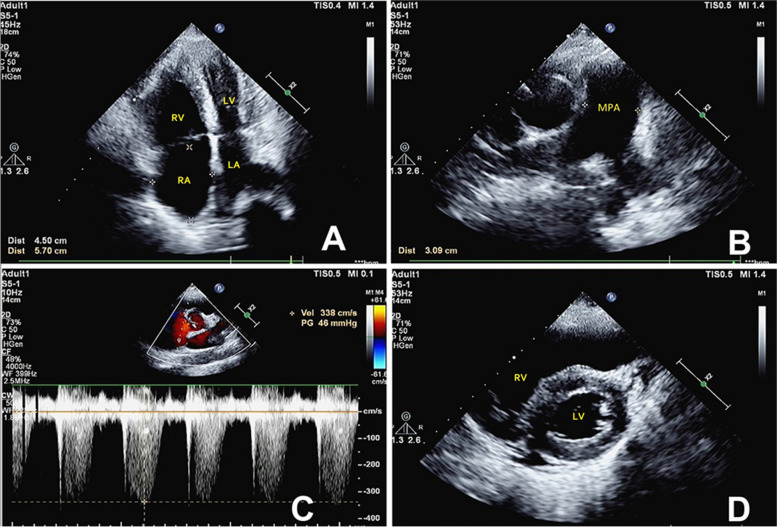
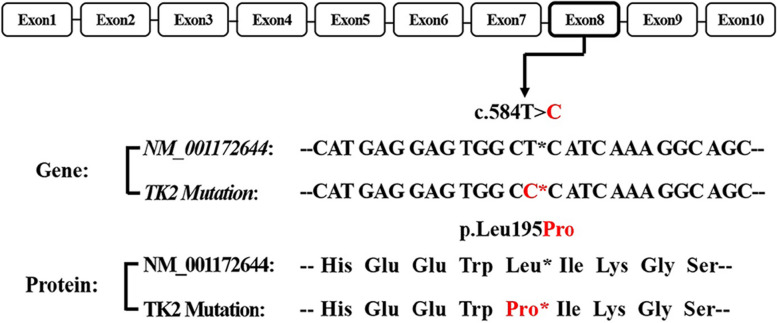
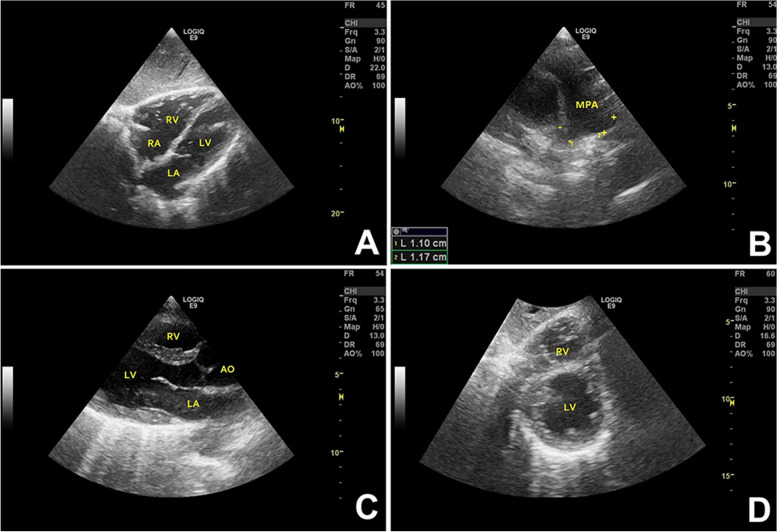
Case presentation: A 49-year-old man presented with clinical features suggestive of MM, i.e., ophthalmoparesis, weakness of the pharyngeal and extremity muscles, and respiratory muscles which gradually progressed to respiratory insufficiency. He had a family history of mitochondrial myopathy. He had increased levels of serum creatine kinase and lactate. Muscle biopsy of left lateral thigh revealed 8% ragged red fibers (RRF) and 42% COX-negative fibers. Gene sequencing revealed a novel heterozygote TK2 variant (NM_001172644: c.584T>C, p.Leu195Pro) and another heterozygous variant (NM_004614.4:c.156+958G>A; rs1965661603) in the intron of TK2 gene. Based on these findings, we diagnosed the patient as a case of MM. Echocardiography revealed right heart enlargement, pulmonary hypertension, left ventricular hypertrophy, and thickening of the main pulmonary artery and its branches. The patient received non-invasive ventilation and coenzyme Q10 (CoQ10). The cardiac structure and function were restored at 1-month follow-up.
Conclusions: This is the first report of reversible cardiac function impairment and left ventricular hypertrophy in a case of adult-onset MM, nocturnal hypoxia is a potential mechanism for left ventricular hypertrophy in patients with MM.
Keywords: Heart failure; Left ventricular hypertrophy; Mitochondrial myopathy; Pulmonary artery hypertension; Respiratory failure.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Mitochondrial DNA depletion in single fibers in a patient with novel TK2 mutations.Neuromuscul Disord. 2014 Aug;24(8):713-20. doi: 10.1016/j.nmd.2014.05.009. Epub 2014 May 29. Neuromuscul Disord. 2014. PMID: 24953930
-
Mitochondrial Myopathy in a 21-Year-Old Man Presenting With Bilateral Lower Extremity Weakness and Swelling.J Prim Care Community Health. 2023 Jan-Dec;14:21501319231172697. doi: 10.1177/21501319231172697. J Prim Care Community Health. 2023. PMID: 37162197 Free PMC article.
-
Adult cases of mitochondrial DNA depletion due to TK2 defect: an expanding spectrum.Neurology. 2012 Feb 28;78(9):644-8. doi: 10.1212/WNL.0b013e318248df2b. Epub 2012 Feb 15. Neurology. 2012. PMID: 22345218
-
Diagnosis of mitochondrial myopathies.Mol Genet Metab. 2013 Sep-Oct;110(1-2):35-41. doi: 10.1016/j.ymgme.2013.07.007. Epub 2013 Jul 17. Mol Genet Metab. 2013. PMID: 23911206 Review.
-
[Mitochondrial myopathy with autosomal dominant inheritance--report of a family and review of the literature].Rinsho Shinkeigaku. 1993 Feb;33(2):162-8. Rinsho Shinkeigaku. 1993. PMID: 8319387 Review. Japanese.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
