

A generalizable and interpretable model for mortality risk stratification of sepsis patients in intensive care unit
- PMID: 37715194
- PMCID: PMC10503007
- DOI: 10.1186/s12911-023-02279-0
A generalizable and interpretable model for mortality risk stratification of sepsis patients in intensive care unit
Abstract
Purpose: This study aimed to construct a mortality model for the risk stratification of intensive care unit (ICU) patients with sepsis by applying a machine learning algorithm.
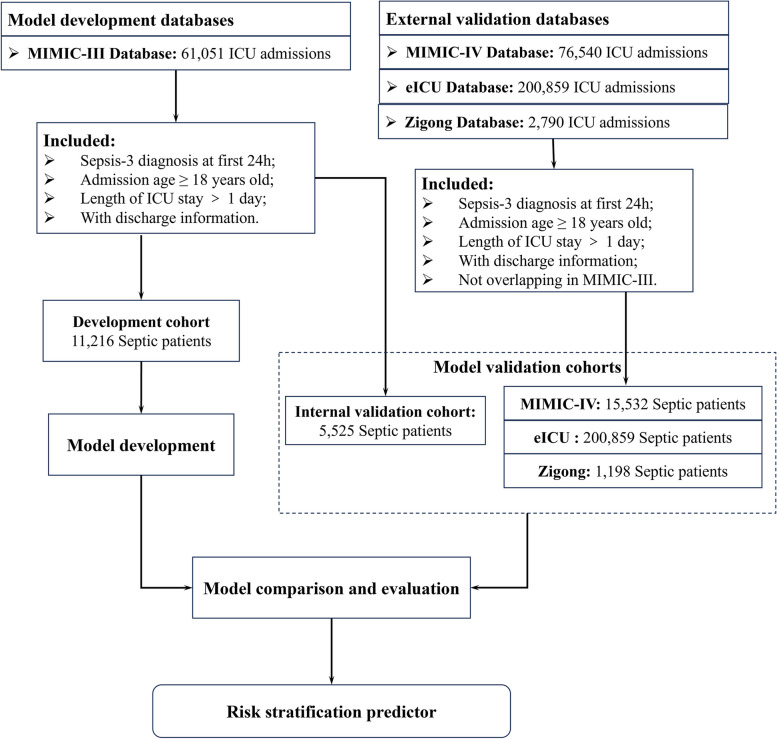
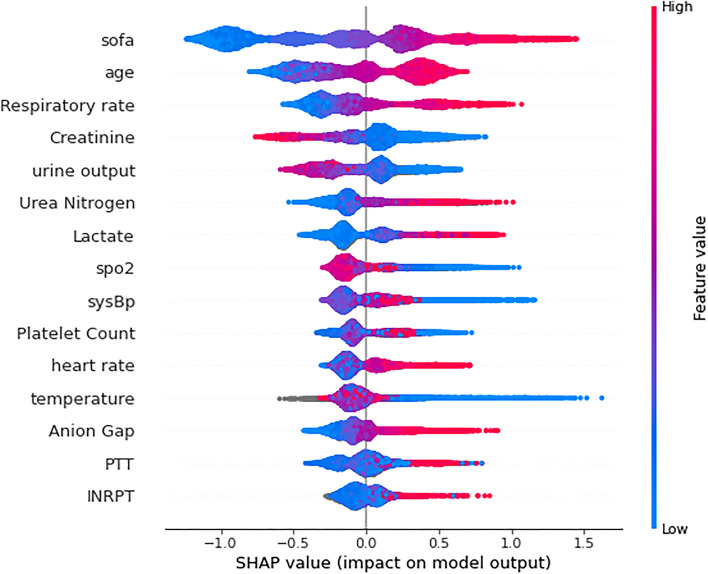
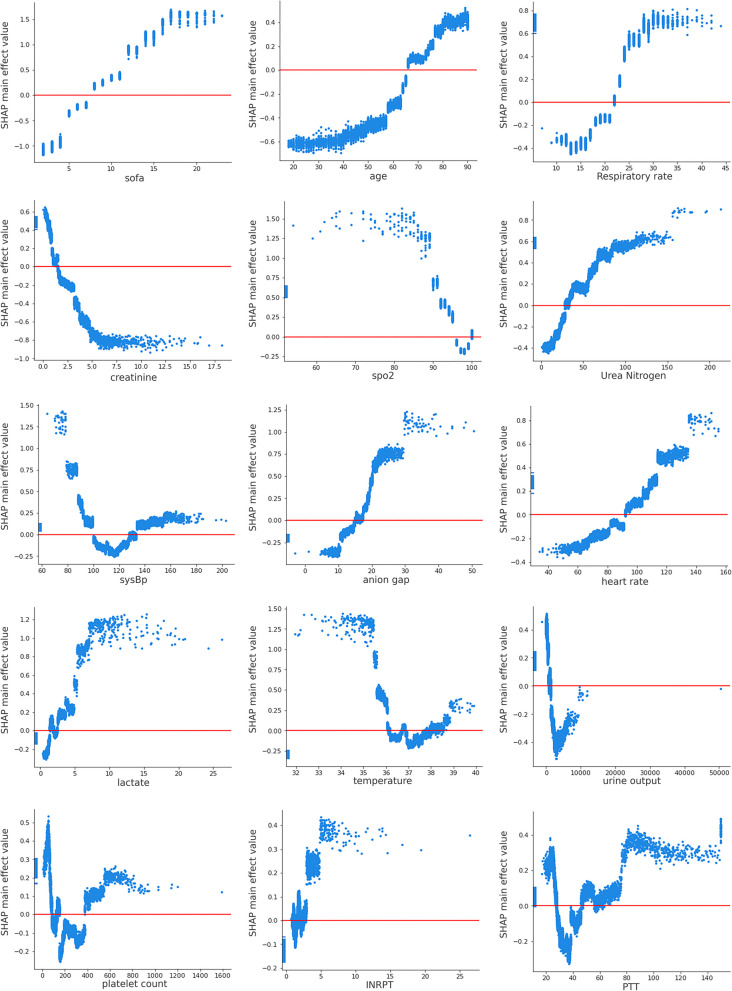
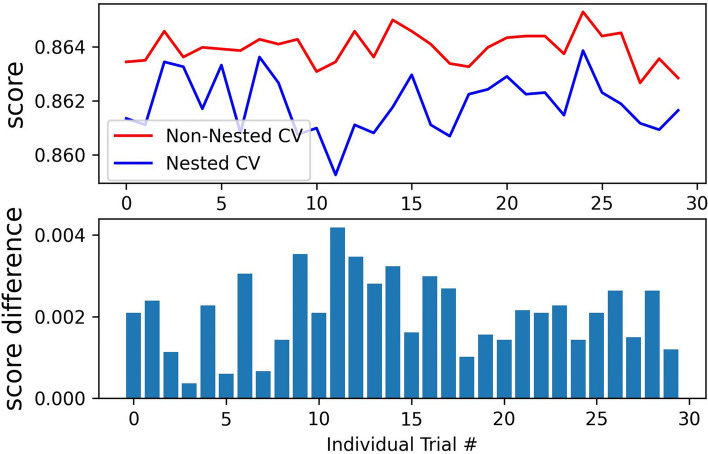
Methods: Adult patients who were diagnosed with sepsis during admission to ICU were extracted from MIMIC-III, MIMIC-IV, eICU, and Zigong databases. MIMIC-III was used for model development and internal validation. The other three databases were used for external validation. Our proposed model was developed based on the Extreme Gradient Boosting (XGBoost) algorithm. The generalizability, discrimination, and validation of our model were evaluated. The Shapley Additive Explanation values were used to interpret our model and analyze the contribution of individual features.
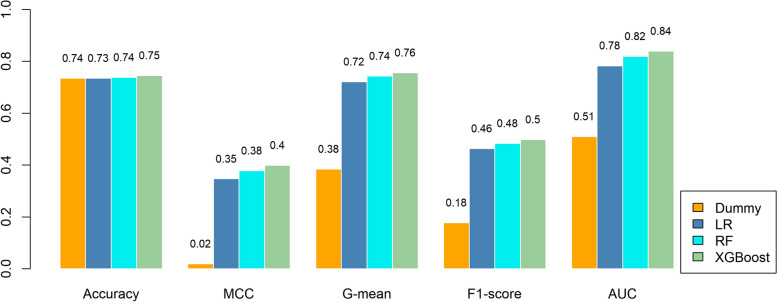
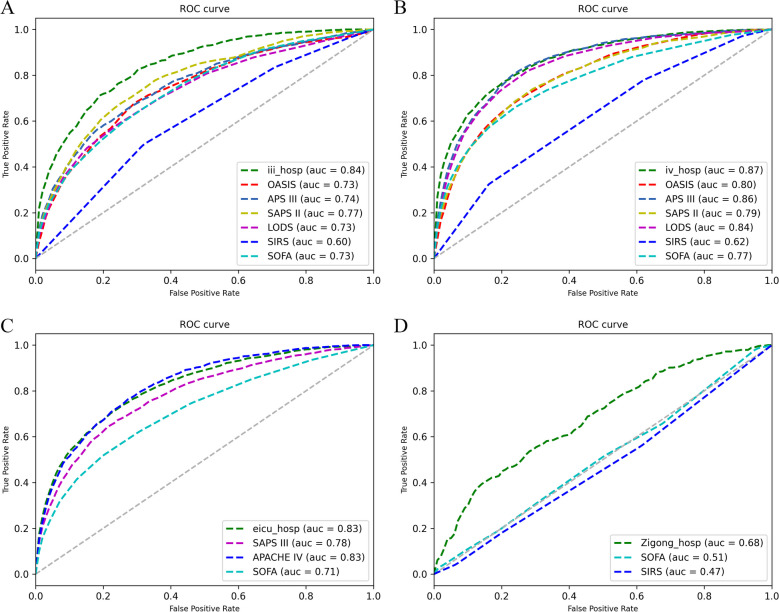
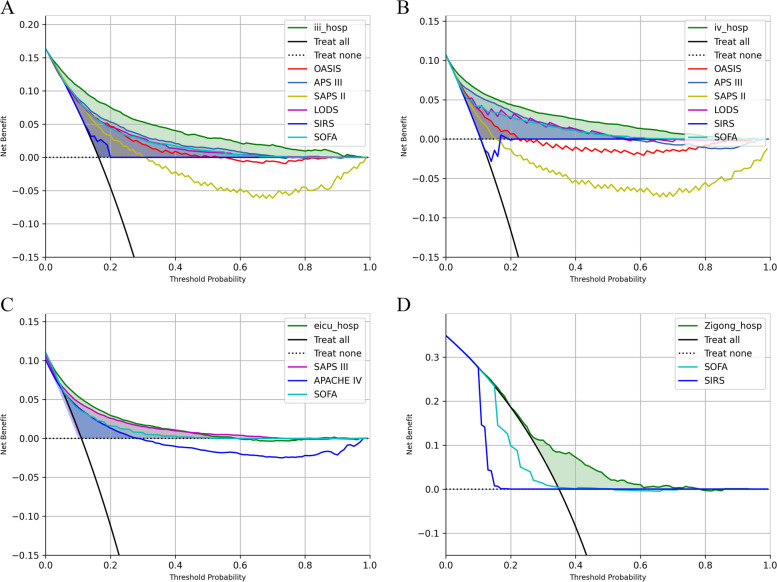
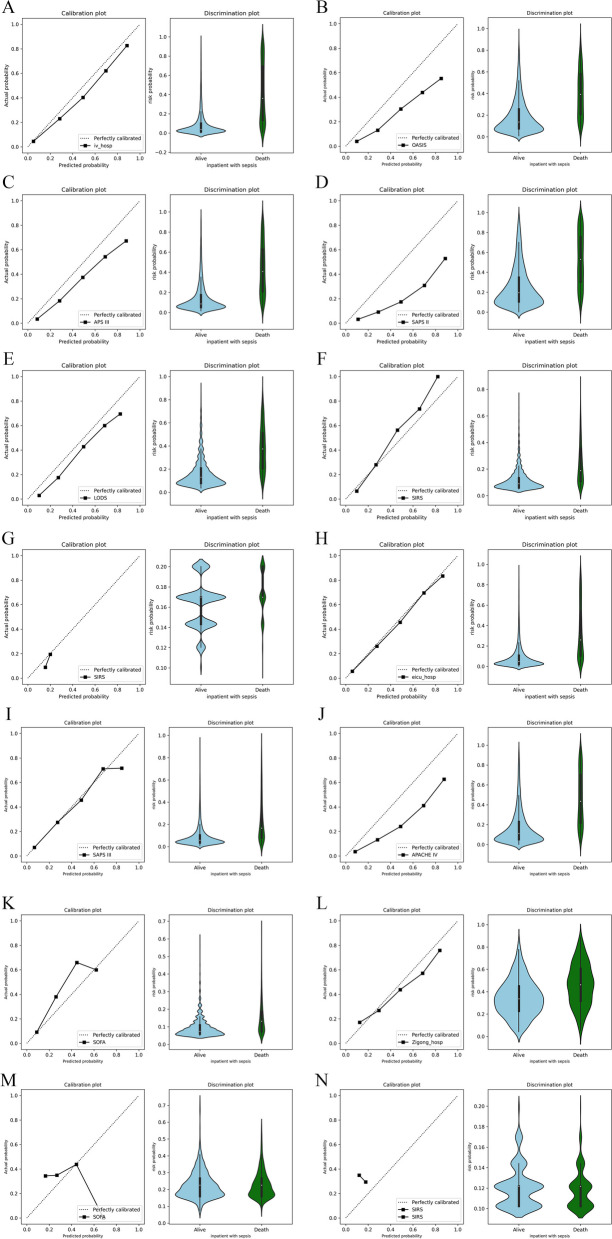
Results: A total of 16,741, 15,532, 22,617, and 1,198 sepsis patients were extracted from the MIMIC-III, MIMIC-IV, eICU, and Zigong databases, respectively. The proposed model had an area under the receiver operating characteristic curve (AUROC) of 0.84 in the internal validation, which outperformed all the traditional scoring systems. In the external validations, the AUROC was 0.87 in the MIMIC-IV database, better than all the traditional scoring systems; the AUROC was 0.83 in the eICU database, higher than the Simplified Acute Physiology Score III and Sequential Organ Failure Assessment (SOFA),equal to 0.83 of the Acute Physiology and Chronic Health Evaluation IV (APACHE-IV), and the AUROC was 0.68 in the Zigong database, higher than those from the systemic inflammatory response syndrome and SOFA. Furthermore, the proposed model showed the best discriminatory and calibrated capabilities and had the best net benefit in each validation.
Conclusions: The proposed algorithm based on XGBoost and SHAP-value feature selection had high performance in predicting the mortality of sepsis patients within 24 h of ICU admission.
Keywords: In-ICU mortality; Multi-source data; Risk stratification; SHAP; Sepsis; XGBoost.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Interpretable machine learning model for early prediction of 28-day mortality in ICU patients with sepsis-induced coagulopathy: development and validation.Eur J Med Res. 2024 Jan 3;29(1):14. doi: 10.1186/s40001-023-01593-7. Eur J Med Res. 2024. PMID: 38172962 Free PMC article.
-
Machine learning-based in-hospital mortality risk prediction tool for intensive care unit patients with heart failure.Front Cardiovasc Med. 2023 Apr 3;10:1119699. doi: 10.3389/fcvm.2023.1119699. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37077747 Free PMC article.
-
An interpretable machine learning model for predicting 28-day mortality in patients with sepsis-associated liver injury.PLoS One. 2024 May 20;19(5):e0303469. doi: 10.1371/journal.pone.0303469. eCollection 2024. PLoS One. 2024. PMID: 38768153 Free PMC article.
-
Methodological Review of Classification Trees for Risk Stratification: An Application Example in the Obesity Paradox.Nutrients. 2025 May 31;17(11):1903. doi: 10.3390/nu17111903. Nutrients. 2025. PMID: 40507172 Free PMC article. Review.
-
Machine Learning Models in Sepsis Outcome Prediction for ICU Patients: Integrating Routine Laboratory Tests-A Systematic Review.Biomedicines. 2024 Dec 19;12(12):2892. doi: 10.3390/biomedicines12122892. Biomedicines. 2024. PMID: 39767798 Free PMC article. Review.
Cited by
-
Harness machine learning for multiple prognoses prediction in sepsis patients: evidence from the MIMIC-IV database.BMC Med Inform Decis Mak. 2025 Mar 31;25(1):152. doi: 10.1186/s12911-025-02976-y. BMC Med Inform Decis Mak. 2025. PMID: 40165185 Free PMC article.
-
Machine learning models for mortality prediction in critically ill patients with acute pancreatitis-associated acute kidney injury.Clin Kidney J. 2024 Sep 11;17(10):sfae284. doi: 10.1093/ckj/sfae284. eCollection 2024 Oct. Clin Kidney J. 2024. PMID: 39385947 Free PMC article.
-
Investigating computational models for diagnosis and prognosis of sepsis based on clinical parameters: Opportunities, challenges, and future research directions.J Intensive Med. 2024 Jul 10;4(4):468-477. doi: 10.1016/j.jointm.2024.04.006. eCollection 2024 Oct. J Intensive Med. 2024. PMID: 39310065 Free PMC article. Review.
References
-
- Organization WH . Global report on the epidemiology and burden of sepsis: current evidence, identifying gaps and future directions. 2020.
-
- Hamilton F, Arnold D, Baird A, Albur M, Whiting P. Early Warning Scores do not accurately predict mortality in sepsis: A meta-analysis and systematic review of the literature. J Infect. 2018;76(3):241–248. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
