

Prospective association between an obesogenic dietary pattern in early adolescence and metabolomics derived and traditional cardiometabolic risk scores in adolescents and young adults from the ALSPAC cohort
- PMID: 37715209
- PMCID: PMC10504726
- DOI: 10.1186/s12986-023-00754-z
Prospective association between an obesogenic dietary pattern in early adolescence and metabolomics derived and traditional cardiometabolic risk scores in adolescents and young adults from the ALSPAC cohort
Abstract
Background: Dietary intake during early life may be a modifying factor for cardiometabolic risk (CMR). Metabolomic profiling may enable more precise identification of CMR in adolescence than traditional CMR scores. We aim to assess and compare the prospective associations between an obesogenic dietary pattern (DP) score at age 13 years with a novel vs. traditional CMR score in adolescence and young adulthood in the Avon Longitudinal Study of Parents and Children (ALSPAC).
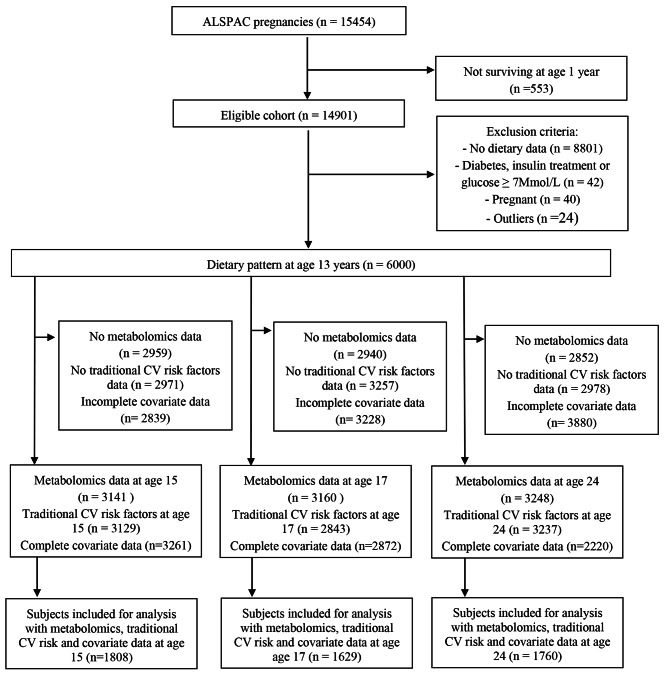
Methods: Study participants were ALSPAC children with diet diary data at age 13. The obesogenic DP z-score, characterized by high energy-density, high % of energy from total fat and free sugars, and low fibre density, was previously derived using reduced rank regression. CMR scores were calculated by combining novel metabolites or traditional risk factors (fat mass index, insulin resistance, mean arterial blood pressure, triacylglycerol, HDL and LDL cholesterol) at age 15 (n = 1808), 17 (n = 1629), and 24 years (n = 1760). Multivariable linear regression models estimated associations of DP z-score with log-transformed CMR z-scores.
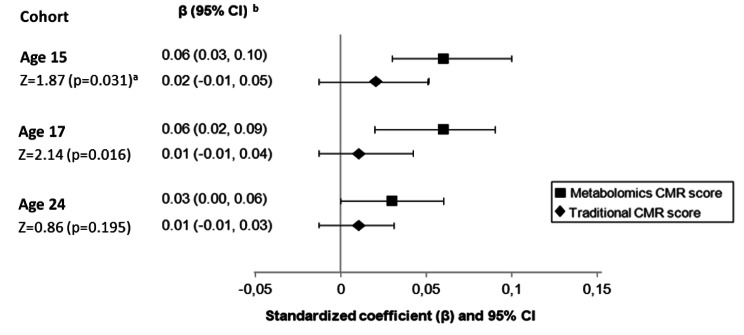
Results: Compared to the lowest tertile, the highest DP z-score tertile at age 13 was associated with an increase in the metabolomics CMR z-score at age 15 (β = 0.20, 95% CI 0.09, 0.32, p trend < 0.001) and at age 17 (β = 0.22, 95% CI 0.10, 0.34, p trend < 0.001), and with the traditional CMR z-score at age 15 (β = 0.15, 95% CI 0.05, 0.24, p trend 0.020). There was no evidence of an association at age 17 for the traditional CMR z-score (β = 0.07, 95% CI -0.03, 0.16, p trend 0.137) or for both scores at age 24.
Conclusions: An obesogenic DP was associated with greater CMR in adolescents. Stronger associations were observed with a novel metabolite CMR score compared to traditional risk factors. There may be benefits from modifying diet during adolescence for CMR health, which should be prioritized for further research in trials.
Keywords: ALSPAC; Adolescence; Cardiometabolic risk; Dietary pattern; Metabolomics.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The inflammatory potential of the diet in childhood is associated with cardiometabolic risk in adolescence/young adulthood in the ALSPAC birth cohort.Eur J Nutr. 2022 Oct;61(7):3471-3486. doi: 10.1007/s00394-022-02860-9. Epub 2022 May 20. Eur J Nutr. 2022. PMID: 35596006 Free PMC article.
-
Prospective association between a Mediterranean-style dietary score in childhood and cardiometabolic risk in young adults from the ALSPAC birth cohort.Eur J Nutr. 2022 Mar;61(2):737-752. doi: 10.1007/s00394-021-02652-7. Epub 2021 Sep 17. Eur J Nutr. 2022. PMID: 34532761 Free PMC article.
-
Prospective association between adherence to UK dietary guidelines in school-age children and cardiometabolic risk markers in adolescence/early adulthood in the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort.Br J Nutr. 2023 Nov 28;130(10):1766-1778. doi: 10.1017/S0007114523000685. Epub 2023 Apr 17. Br J Nutr. 2023. PMID: 37066640 Free PMC article.
-
Lipid Screening in Childhood for Detection of Multifactorial Dyslipidemia: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Aug. Report No.: 14-05204-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Aug. Report No.: 14-05204-EF-1. PMID: 27559550 Free Books & Documents. Review.
-
Adolescent cardiometabolic risk scores: A scoping review.Nutr Metab Cardiovasc Dis. 2022 Dec;32(12):2669-2676. doi: 10.1016/j.numecd.2022.08.022. Epub 2022 Sep 6. Nutr Metab Cardiovasc Dis. 2022. PMID: 36153209
Cited by
-
Associations of childhood diet quality scores with arterial stiffness and carotid artery intima-media thickness in adolescence/early adulthood: findings from the ALSPAC cohort.Br J Nutr. 2024 Feb 28;131(4):720-735. doi: 10.1017/S0007114523002763. Epub 2024 Jan 5. Br J Nutr. 2024. PMID: 38178807 Free PMC article.
-
Investigating eating architecture and the impact of the precision of recorded eating time: a cross-sectional study.Am J Clin Nutr. 2025 Mar;121(3):685-694. doi: 10.1016/j.ajcnut.2025.01.012. Epub 2025 Jan 11. Am J Clin Nutr. 2025. PMID: 39805560 Free PMC article.
References
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of Disease Study 2017. The Lancet. 2018;392(10159):1736–88. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
