

Predictors of persisting pain in children with Juvenile Idiopathic Arthritis: a case control study nested in the ReACCh-Out cohort
- PMID: 37715224
- PMCID: PMC10504744
- DOI: 10.1186/s12969-023-00885-w
Predictors of persisting pain in children with Juvenile Idiopathic Arthritis: a case control study nested in the ReACCh-Out cohort
Abstract
Background: To identify baseline predictors of persisting pain in children with Juvenile Idiopathic Arthritis (JIA), relative to patients with JIA who had similar baseline levels of pain but in whom the pain did not persist.
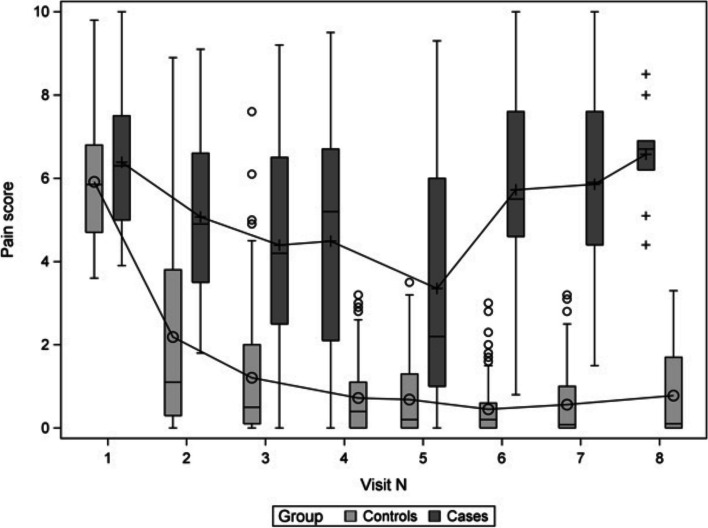
Methods: We used data from the Research in Arthritis in Canadian Children emphasizing Outcomes (ReACCh-Out) inception cohort to compare cases of 'moderate persisting pain' with controls of 'moderate decreasing pain'. Moderate pain was defined as a Visual Analogue Scale (VAS) for pain measurement score of > 3.5 cm. Follow-up was minimum 3 years. Univariate and Multivariate logistic regression models ascertained baseline predictors of persisting pain.
Results: A total of 31 cases and 118 controls were included. Mean pain scores at baseline were 6.4 (SD 1.6) for cases and 5.9 (1.5) for controls. A greater proportion of cases than controls were females (77.4% vs 65.0%) with rheumatoid factor positive polyarthritis (12.9% vs 4.2%) or undifferentiated JIA (22.6% vs 8.5%). Oligoarthritis was less frequent in cases than controls (9.7% vs 33%). At baseline, cases had more active joints (mean of 11.4 vs 7.7) and more sites of enthesitis (4.6 vs 0.7) than controls. In the final multivariate regression model, enthesitis count at baseline (OR 1.40, CI 95% 1.19-1.76), female sex (4.14, 1.33-16.83), and the overall Quality of My Life (QoML) baseline score (0.82, 0.69-0.98) predicted development of persisting pain.
Conclusions: Among newly diagnosed children with JIA with moderate pain, female sex, lower overall quality of life, and higher enthesitis counts at baseline predicted development of persisting pain. If our findings are confirmed, patients with these characteristics may be candidates for interventions to prevent development of chronic pain.
Keywords: Children; Enthesitis; Juvenile idiopathic arthritis; Pain; Quality of life.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
There has been no financial support or other benefits from commercial sources for the work reported on in this manuscript. NJS is an employee of Janssen Scientific Affairs, LLC and owns Abbvie, Gilead, Iovance stock. The other authors have no financial interests which could create a potential conflict of interest or the appearance of a conflict of interest regarding the work.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
