

Prevalence and Predictors of Barrett's Esophagus After Negative Initial Endoscopy: Analysis From Two National Databases
- PMID: 37716614
- PMCID: PMC10922211
- DOI: 10.1016/j.cgh.2023.08.035
Prevalence and Predictors of Barrett's Esophagus After Negative Initial Endoscopy: Analysis From Two National Databases
Abstract
Background & aims: Guidelines suggest a single screening esophagogastroduodenoscopy (EGD) in patients with multiple risk factors for Barrett's esophagus (BE). We aimed to determine BE prevalence and predictors on repeat EGD after a negative initial EGD, using 2 large national databases (GI Quality Improvement Consortium [GIQuIC] and TriNetX).
Methods: Patients who underwent at least 2 EGDs were included and those with BE or esophageal adenocarcinoma detected at initial EGD were excluded. Patient demographics and prevalence of BE on repeat EGD were collected. Multivariate logistic regression was performed to assess for independent risk factors for BE detected on the repeat EGD.
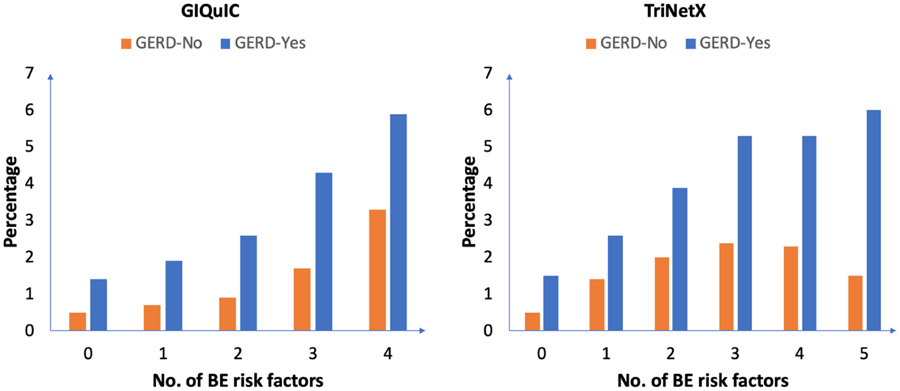
Results: In 214,318 and 153,445 patients undergoing at least 2 EGDs over a median follow-up of 28-35 months, the prevalence of BE on repeat EGD was 1.7% in GIQuIC and 3.4% in TriNetX, respectively (26%-45% of baseline BE prevalence). Most (89%) patients had nondysplastic BE. The prevalence of BE remained stable over time (from 1 to >5 years from negative initial EGD) but increased with increasing number of risk factors. BE prevalence in a high-risk population (gastroesophageal reflux disease plus ≥1 risk factor for BE) was 3%-4%.
Conclusions: In this study of >350,000 patients, rates of BE on repeat EGD ranged from 1.7%-3.4%, and were higher in those with multiple risk factors. Most were likely missed at initial evaluation, underscoring the importance of a high-quality initial endoscopic examination. Although routine repeat endoscopic BE screening after a negative initial examination is not recommended, repeat screening may be considered in carefully selected patients with gastroesophageal reflux disease and ≥2 risk factors for BE, potentially using nonendoscopic tools.
Keywords: Endoscopy; Esophageal adenocarcinoma; Screening.
Copyright © 2024 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Cameron A, Ott B, Payne W. The incidence of adenocarcinoma in columnar-lined (Barrett's) esophagus. N Engl J Med. 1985;313:857–9. - PubMed
-
- Holmes RS, Vaughan TL. Epidemiology and pathogenesis of esophageal cancer. Semin Radiat Oncol. 2007;17:2–9. - PubMed
-
- Pohl H, Sirovich B, Welch HG. Esophageal adenocarcinoma incidence:Are we reaching the peak?. Cancer Epidemiol Biomarkers Prev 2010;19:1468–70. - PubMed
-
- Siegel RL, Miller KD, Jemal A: Cancer statistics, 2019. Cancer J Clin 2019; 69: pp. 7–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
