

Phototherapy Restores Deficient Type I IFN Production and Enhances Antitumor Responses in Mycosis Fungoides
- PMID: 37716650
- PMCID: PMC10922223
- DOI: 10.1016/j.jid.2023.06.212
Phototherapy Restores Deficient Type I IFN Production and Enhances Antitumor Responses in Mycosis Fungoides
Abstract
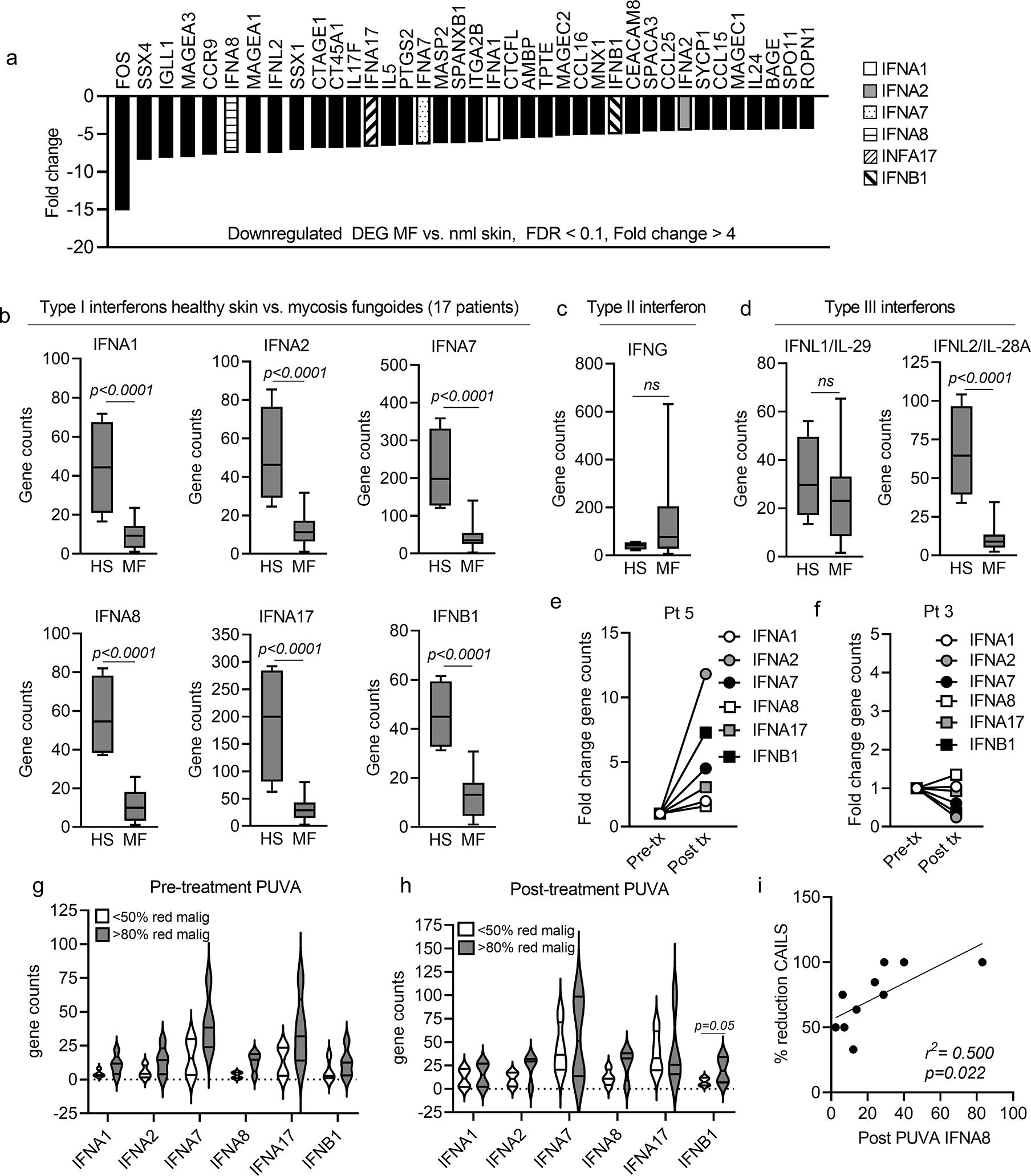
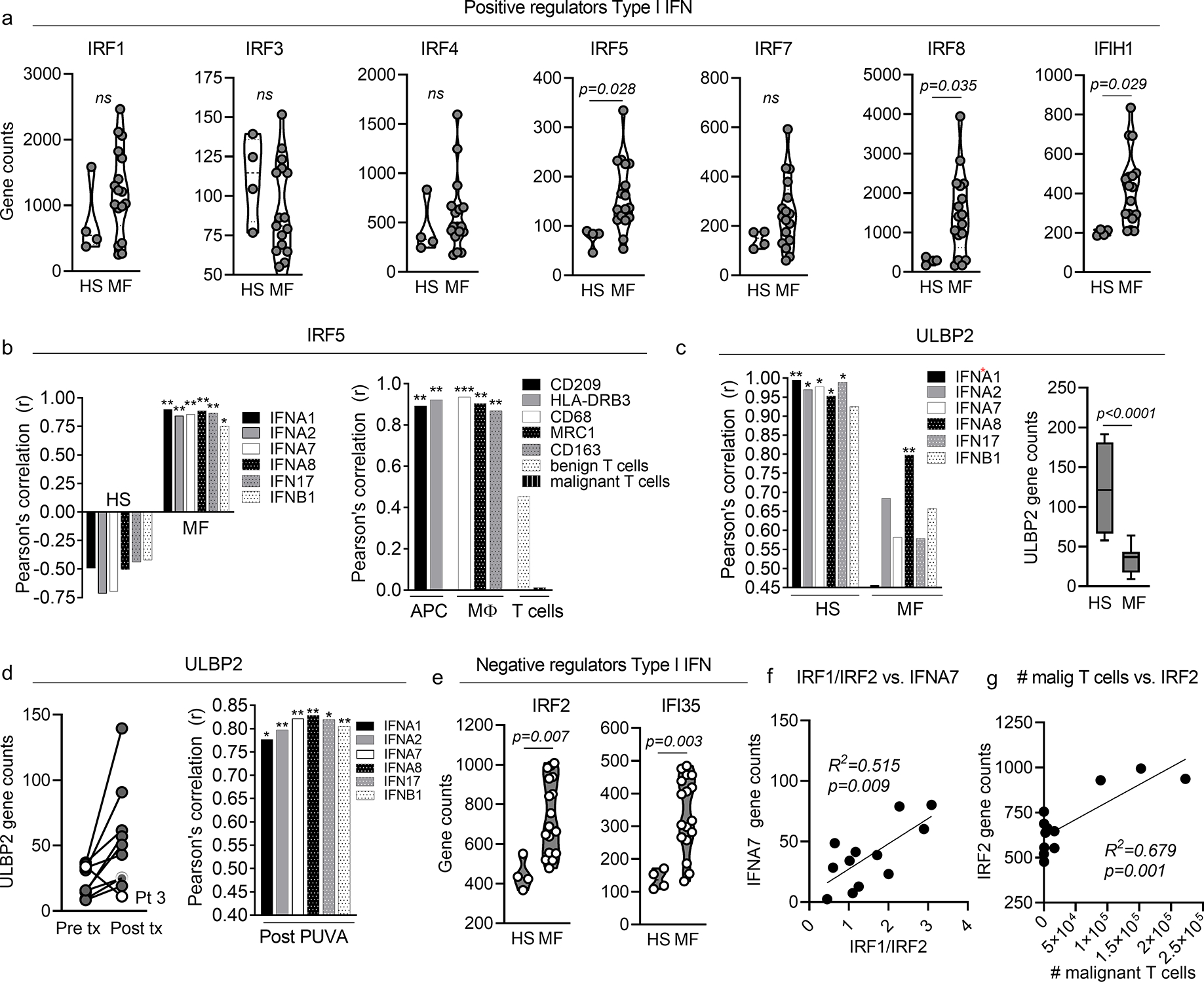
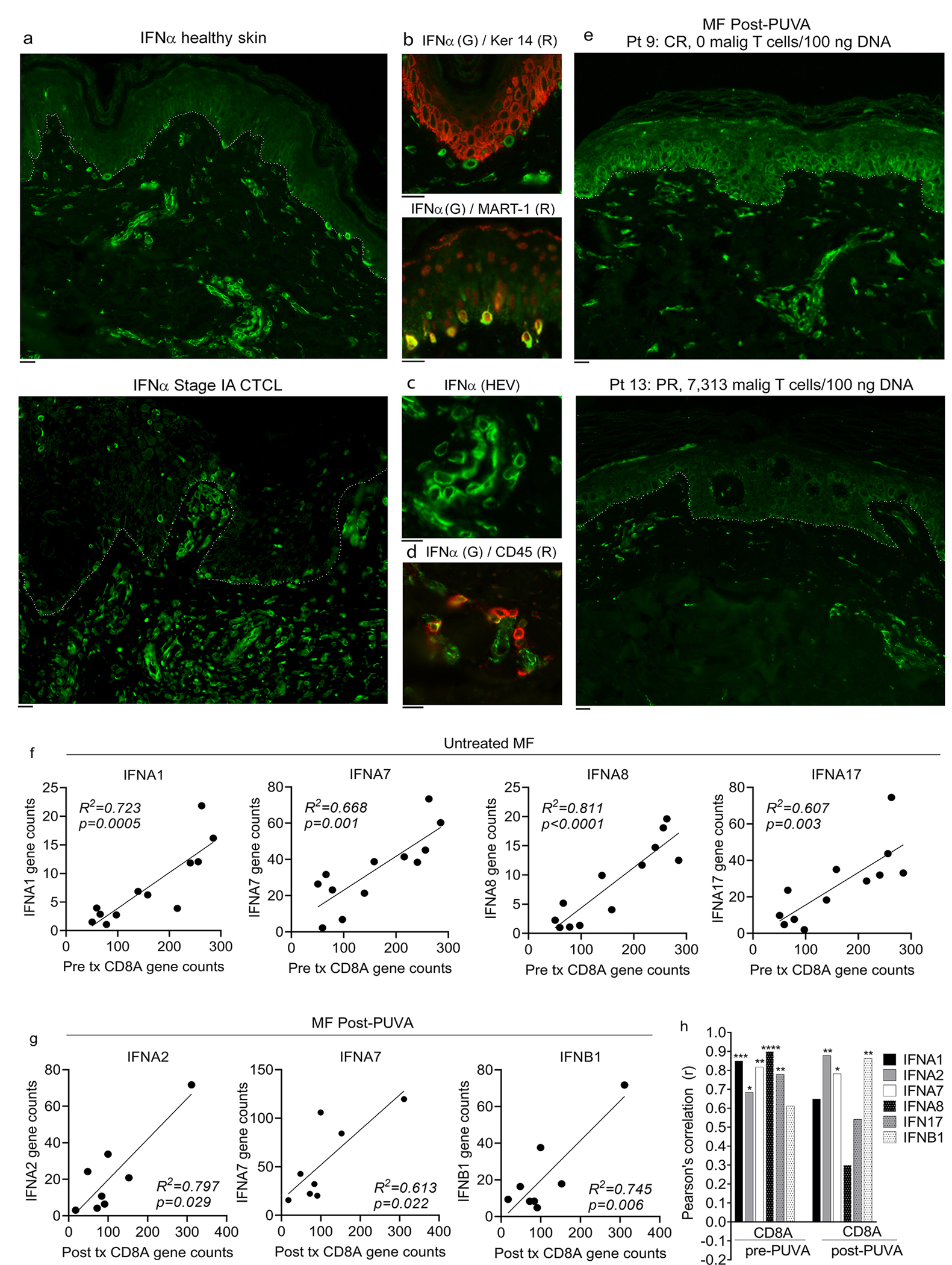
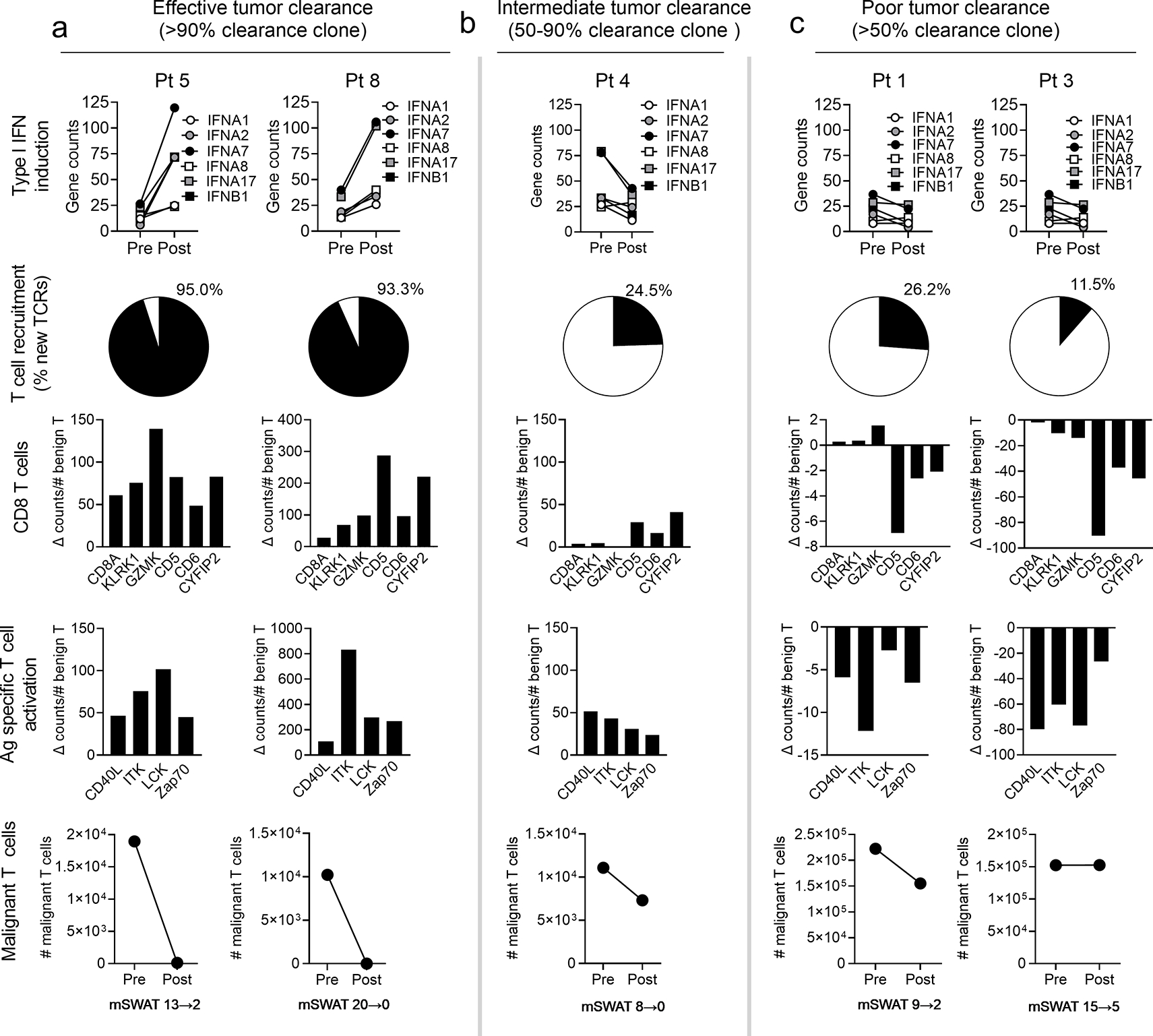
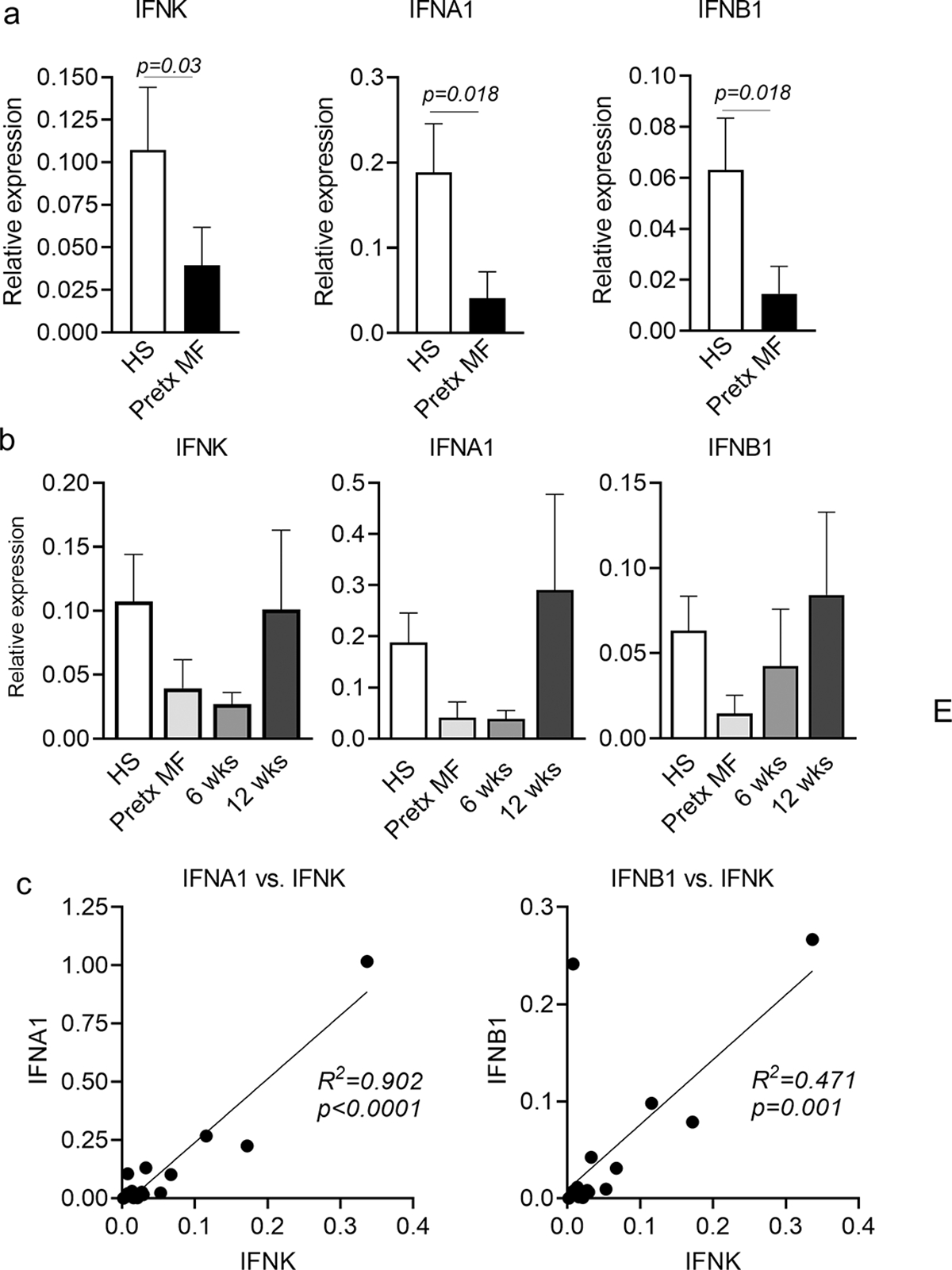
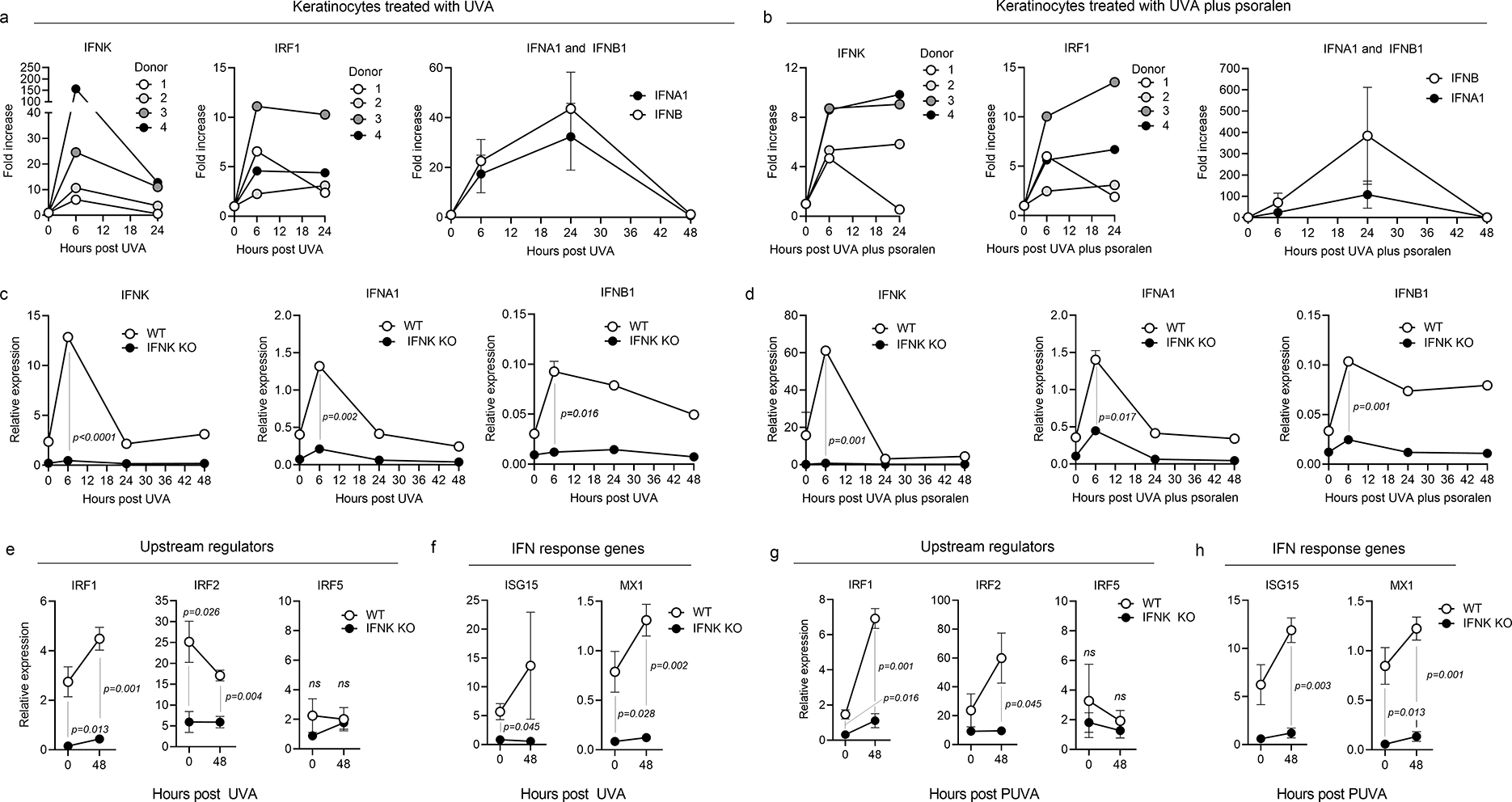
Transcriptional profiling demonstrated markedly reduced type I IFN gene expression in untreated mycosis fungoides (MF) skin lesions compared with that in healthy skin. Type I IFN expression in MF correlated with antigen-presenting cell-associated IRF5 before psoralen plus UVA therapy and epithelial ULBP2 after therapy, suggesting an enhancement of epithelial type I IFN. Immunostains confirmed reduced baseline type I IFN production in MF and increased levels after psoralen plus UVA treatment in responding patients. Effective tumor clearance was associated with increased type I IFN expression, enhanced recruitment of CD8+ T cells into skin lesions, and expression of genes associated with antigen-specific T-cell activation. IFNk, a keratinocyte-derived inducer of type I IFNs, was increased by psoralen plus UVA therapy and expression correlated with upregulation of other type I IFNs. In vitro, deletion of keratinocyte IFNk decreased baseline and UVA-induced expression of type I IFN and IFN response genes. In summary, we find a baseline deficit in type I IFN production in MF that is restored by psoralen plus UVA therapy and correlates with enhanced antitumor responses. This may explain why MF generally develops in sun-protected skin and suggests that drugs that increase epithelial type I IFNs, including topical MEK and EGFR inhibitors, may be effective therapies for MF.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Psoralen Plus UVA Induces Local IFN Production and Antitumor Responses in Cutaneous T-Cell Lymphoma.J Invest Dermatol. 2024 Mar;144(3):449-450. doi: 10.1016/j.jid.2023.08.029. Epub 2023 Nov 3. J Invest Dermatol. 2024. PMID: 37921716 No abstract available.
Similar articles
-
Phototherapy of Mycosis Fungoides.Dermatol Clin. 2015 Oct;33(4):697-702. doi: 10.1016/j.det.2015.05.005. Epub 2015 Aug 1. Dermatol Clin. 2015. PMID: 26433842 Review.
-
Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): part II. Prognosis, management, and future directions.J Am Acad Dermatol. 2014 Feb;70(2):223.e1-17; quiz 240-2. doi: 10.1016/j.jaad.2013.08.033. J Am Acad Dermatol. 2014. PMID: 24438970 Review.
-
Photochemotherapy for mycosis fungoides.Arch Dermatol. 1977 Aug;113(8):1047-51. Arch Dermatol. 1977. PMID: 889332
-
Interventions for mycosis fungoides.Cochrane Database Syst Rev. 2020 Jul 7;7(7):CD008946. doi: 10.1002/14651858.CD008946.pub3. Cochrane Database Syst Rev. 2020. PMID: 32632956 Free PMC article.
-
PUVA-induced pityriasis lichenoides chronica-like papular lesions in patients with mycosis fungoides: a clinical, histopathological and immunohistochemical study.Arch Dermatol Res. 2019 Nov;311(9):673-678. doi: 10.1007/s00403-019-01949-2. Epub 2019 Jul 12. Arch Dermatol Res. 2019. PMID: 31300833 Clinical Trial.
Cited by
-
The Role of Cytokines in Cutaneous T Cell Lymphoma: A Focus on the State of the Art and Possible Therapeutic Targets.Cells. 2024 Mar 28;13(7):584. doi: 10.3390/cells13070584. Cells. 2024. PMID: 38607023 Free PMC article. Review.
-
Modulation of the skin microbiome in cutaneous T-cell lymphoma delays tumour growth and increases survival in the murine EL4 model.Front Immunol. 2024 Apr 5;15:1255859. doi: 10.3389/fimmu.2024.1255859. eCollection 2024. Front Immunol. 2024. PMID: 38646524 Free PMC article.
-
Vitamin D in Cutaneous T-Cell Lymphoma.Cells. 2024 Mar 13;13(6):503. doi: 10.3390/cells13060503. Cells. 2024. PMID: 38534347 Free PMC article. Review.
References
-
- Agar NS, Wedgeworth E, Crichton S, Mitchell TJ, Cox M, Ferreira S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sezary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2010;28(31):4730–9. - PubMed
-
- Akiyama Y, Kondou R, Iizuka A, Ohshima K, Urakami K, Nagashima T, et al. Immune response-associated gene analysis of 1,000 cancer patients using whole-exome sequencing and gene expression profiling-Project HOPE. Biomed Res 2016;37(4):233–42. - PubMed
-
- Buhl T, Schön MP. Peeking into immunoregulatory effects of phototherapy. Experimental dermatology 2016. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
