

A Comparative Study on Graft and Overall Survival Rates Between Diabetic and Nondiabetic Kidney Transplant Patients Through Survival Analysis
- PMID: 37719299
- PMCID: PMC10503289
- DOI: 10.1177/20543581231199011
A Comparative Study on Graft and Overall Survival Rates Between Diabetic and Nondiabetic Kidney Transplant Patients Through Survival Analysis
Abstract
Background: Patients with diabetes mellitus (DM) have worse graft and overall survival, but recent evidence suggests that the difference is no longer significant.
Objective: To compare the outcomes between patients with end-stage kidney disease due to DM (ESKD-DM) and ESKD due to nondiabetic etiology (ESKD-non-DM) who underwent kidney transplantation (KT) up to 10 years of follow-up.
Design: Survival analysis of a retrospective cohort.
Setting and patients: All patients who underwent KT at the Hospital Universitario San Ignacio, Colombia, between 2004 and 2022.
Measurements: Overall and graft survival in ESKD-DM and ESKD-non-DM who received KT. Patients who died with functional graft were censored for the calculation of kidney graft survival.
Methods: Log-rank test, Cox proportional hazards model, and competing risk analysis were used to compare overall and graft survival in patients with ESKD-DM and ESKD-non-DM who underwent KT.
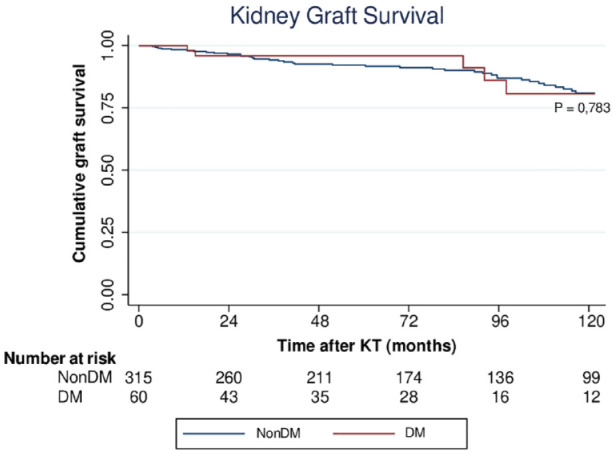
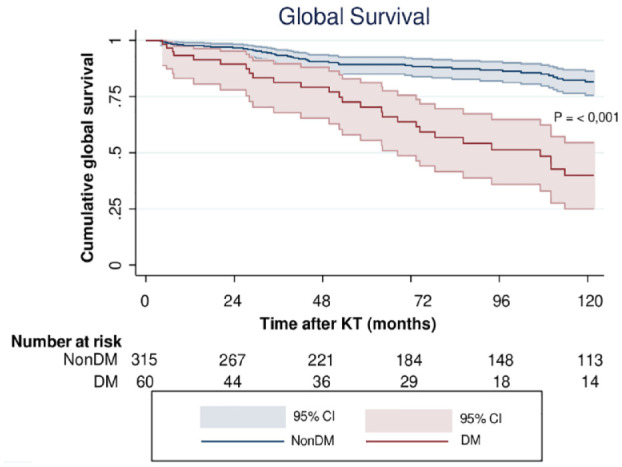
Results: A total of 375 patients were included: 60 (16%) with ESKD-DM and 315 (84%) with ESKD-non-DM. Median follow-up was 83.3 months. Overall survival was lower in patients with ESKD-DM at 5 (75.0% vs 90.8%, P < .001) and 10 years (55.0% vs 86.7%, P < .001). Cardiovascular death was higher in patients with diabetes (27.3% vs 8.2%, P = .021). Death-censored graft survival was similar in both groups (96.7% vs 93.3% at 5 years, P = .324). On multivariate analysis, the factors associated with global survival were DM (hazard ratio [HR] = 2.11, 95% confidence interval [CI] = 1.23-3.60, P = .006), recipient age (HR = 1.05, 95% CI = 1.02-1.08, P < .001), delayed graft function (HR = 2.07, 95% CI = 1.24-3.46, P = .005), and donor age (HR = 1.03, 95% CI = 1.01-1.05, P = .002). In the competing risk analysis, DM was associated with mortality only in the cardiovascular death group (sub-hazard ratio [SHR] = 6.06, 95% CI = 1.01-36.4, P = .049).
Limitations: Change in diabetes treatment received over time and adherence to glycemic targets were not considered. The sample size is relatively small, which limits the precision of our estimates. The Kidney Donor Profile Index and the occurrence of treated acute rejection were not included in the regression models.
Conclusion: Overall survival is lower in patients with diabetes, possibly due to older age and cardiovascular comorbidities. Therefore, patients with diabetes should be followed more closely to control cardiovascular risk factors. However, there is no difference in graft survival.
Contexte: Les patients diabétiques (DB) sont ceux qui présentent les pires résultats de greffe et de survie globale, mais des données récentes suggèrent que la différence n’est désormais plus significative.
Objectif: Comparer les résultats des patients atteints d’insuffisance rénale terminale causée par le DB (IRT-DB) et ceux des patients non-diabétiques (IRT-nonDB) pour une période de 10 ans après une transplantation rénale (TR).
Conception: Analyse de la survie d’une cohorte rétrospective.
Sujets et cadre de l’étude: Tous les patients qui ont subi une TR à l’Hôpital Universitario San Ignacio (Colombie) entre 2004 et 2022.
Mesures: La survie globale et la survie du greffon chez les patients IRT-DB et IRT-nonDB après une TR. Les patients décédés avec un greffon fonctionnel ont été censurés pour le calcul de la survie du greffon.
Méthodologie: Le test logarithmique par rangs, un modèle de régression à effet proportionnel de Cox et une analyse des risques concurrents ont été utilisés pour comparer la survie globale et la survie du greffon des patients atteints d’IRT-DB et d’IRT-nonDB après une TR.
Résultats: Au total, 375 patients ont été inclus à l’étude, soit 60 patients (16 %) atteints d’IRT-DB et 315 (84 %) atteints d’IRT-nonDB. La durée médiane du suivi était de 83,3 mois. La survie globale était plus faible chez les patients atteints d’IRT-DB à 5 ans (75,0 c. 90,8 %; p<0,001) et à 10 ans (55,0 % c. 86,7 %; p<0,001). Les décès de causes cardiovasculaires ont été plus nombreux chez les patients diabétiques (27,3 % c. 8,2 %; p=0,021). La survie du greffon censurée pour le décès était similaire pour les deux groupes (96,7 % c. 93,3 % à 5 ans, p=0,324). Dans l’analyse multivariée, les facteurs associés à la survie globale étaient le DB (RR=2,11; IC95 : 1,23-3,60; p=0,006), l’âge du receveur (RR=1,05; IC95 : 1,02-1,08; p<0,001), le retard de fonction du greffon (RR = 2,07; IC95 : 1,24-3,46; p = 0,005) et l’âge du donneur (RR = 1,03; IC95 : 1,01-1,05; p=0,002). Dans l’analyse des risques concurrents, le DB a été associé à la mortalité uniquement dans le groupe de patients décédés de causes cardiovasculaires (RRS=6,06; IC95 : 1,01-36,4; p=0,049).
Limites: Les modifications dans le traitement du diabète au fil du temps et l’observance des cibles glycémiques n’ont pas été prises en compte. La taille de l’échantillon est relativement faible, ce qui limite la précision des estimations. L’indice de profil du donneur (Kidney Donor Profile Index—KDPI) et la survenue d’un rejet aigu traité n’ont pas été inclus dans les modèles de régression.
Conclusion: La survie globale est plus faible chez les patients diabétiques, peut-être en raison de l’âge avancé et des comorbidités cardiovasculaires de ces patients. Les patients diabétiques devraient par conséquent faire l’objet d’un suivi plus rapproché afin de surveiller les facteurs de risque cardiovasculaire. Aucune différence n’a cependant été observée pour la survie du greffon.
Keywords: cause of death; diabetes mellitus; graft survival; kidney transplantation; patient survival.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Temporal trends of incident diabetes mellitus and subsequent outcomes in patients receiving kidney transplantation: a national cohort study in Taiwan.Diabetol Metab Syndr. 2020 Apr 28;12:34. doi: 10.1186/s13098-020-00541-3. eCollection 2020. Diabetol Metab Syndr. 2020. PMID: 32368254 Free PMC article.
-
Kidney transplantation in type 2 diabetic patients: a matched survival analysis.Transplant Proc. 2013 Jul-Aug;45(6):2141-6. doi: 10.1016/j.transproceed.2012.11.013. Epub 2013 Jun 6. Transplant Proc. 2013. PMID: 23747181
-
Kidney Transplantation Improves Survival in Lupus Nephritis With End-Stage Kidney Disease.Kidney Int Rep. 2025 Feb 3;10(4):1163-1174. doi: 10.1016/j.ekir.2025.01.034. eCollection 2025 Apr. Kidney Int Rep. 2025. PMID: 40303207 Free PMC article.
-
Long-term outcomes of end-stage kidney disease for patients with IgA nephropathy: A multi-centre registry study.Nephrology (Carlton). 2016 May;21(5):387-96. doi: 10.1111/nep.12629. Nephrology (Carlton). 2016. PMID: 26393772
-
Kidney and liver organ transplantation in persons with human immunodeficiency virus: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2010;10(4):1-56. Epub 2010 Mar 1. Ont Health Technol Assess Ser. 2010. PMID: 23074407 Free PMC article.
Cited by
-
Physical Frailty and Functional Status in Kidney Transplantation: A Systematic Review.Can J Kidney Health Dis. 2024 Dec 16;11:20543581241300777. doi: 10.1177/20543581241300777. eCollection 2024. Can J Kidney Health Dis. 2024. PMID: 39691414 Free PMC article.
-
Mortality risk for kidney transplant candidates with diabetes: a population cohort study.Diabetologia. 2024 Nov;67(11):2530-2538. doi: 10.1007/s00125-024-06245-x. Epub 2024 Aug 6. Diabetologia. 2024. PMID: 39103718 Free PMC article.
-
Diabetes Mellitus in Kidney Transplant Recipients: New Horizons in Treatment.J Clin Med. 2025 Feb 7;14(4):1048. doi: 10.3390/jcm14041048. J Clin Med. 2025. PMID: 40004579 Free PMC article. Review.
References
-
- Saran R, Robinson B, Abbott KC, et al.. US renal data system 2019 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2020;75:A6-A7. - PubMed
-
- Jadoul M, Winkelmayer WC. KDIGO 2022 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020;98:S1-S115. - PubMed
-
- US Renal Data System: United States Renal Data System Annual Data Report: Mortality. Ann Arbor, MI: US Renal Data System; 2015.
LinkOut - more resources
Full Text Sources
