

Disease-specific protein corona formed in pathological intestine enhances the oral absorption of nanoparticles
- PMID: 37719377
- PMCID: PMC10501873
- DOI: 10.1016/j.apsb.2023.02.012
Disease-specific protein corona formed in pathological intestine enhances the oral absorption of nanoparticles
Abstract
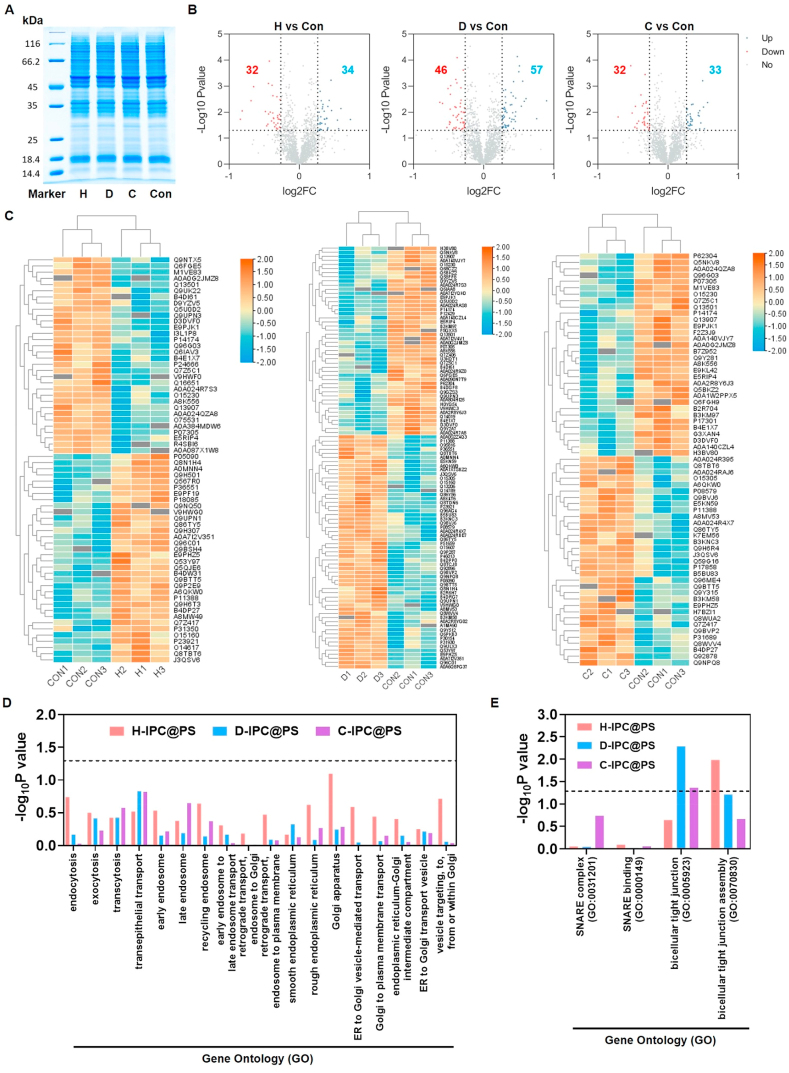
Protein corona (PC) has been identified to impede the transportation of intravenously injected nanoparticles (NPs) from blood circulation to their targeted sites. However, how intestinal PC (IPC) affects the delivery of orally administered NPs are still needed to be elucidated. Here, we found that IPC exerted "positive effect" or "negative effect" depending on different pathological conditions in the gastrointestinal tract. We prepared polystyrene nanoparticles (PS) adsorbed with different IPC derived from the intestinal tract of healthy, diabetic, and colitis rats (H-IPC@PS, D-IPC@PS, C-IPC@PS). Proteomics analysis revealed that, compared with healthy IPC, the two disease-specific IPC consisted of a higher proportion of proteins that were closely correlated with transepithelial transport across the intestine. Consequently, both D-IPC@PS and C-IPC@PS mainly exploited the recycling endosome and ER-Golgi mediated secretory routes for intracellular trafficking, which increased the transcytosis from the epithelium. Together, disease-specific IPC endowed NPs with higher intestinal absorption. D-IPC@PS posed "positive effect" on intestinal absorption into blood circulation for diabetic therapy. Conversely, C-IPC@PS had "negative effect" on colitis treatment because of unfavorable absorption in the intestine before arriving colon. These results imply that different or even opposite strategies to modulate the disease-specific IPC need to be adopted for oral nanomedicine in the treatment of variable diseases.
Keywords: Disease-specific; Intestinal absorption; Intestinal protein corona; Intracellular trafficking; Oral nanoparticles; Pathological intestine; Proteomics analysis; Transepithelial transport.
© 2023 Chinese Pharmaceutical Association and Institute of Materia Medica, Chinese Academy of Medical Sciences. Production and hosting by Elsevier B.V.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







Similar articles
-
Proteomic analysis of intracellular protein corona of nanoparticles elucidates nano-trafficking network and nano-bio interactions.Theranostics. 2020 Jan 1;10(3):1213-1229. doi: 10.7150/thno.38900. eCollection 2020. Theranostics. 2020. PMID: 31938061 Free PMC article.
-
In vitro gastrointestinal digestion increases the translocation of polystyrene nanoparticles in an in vitro intestinal co-culture model.Nanotoxicology. 2015;9(7):886-94. doi: 10.3109/17435390.2014.988664. Epub 2015 Sep 4. Nanotoxicology. 2015. PMID: 25672814
-
Self-Assembled Core-Shell-Type Lipid-Polymer Hybrid Nanoparticles: Intracellular Trafficking and Relevance for Oral Absorption.J Pharm Sci. 2017 Oct;106(10):3120-3130. doi: 10.1016/j.xphs.2017.05.029. Epub 2017 May 27. J Pharm Sci. 2017. PMID: 28559042
-
Protein corona formed in the gastrointestinal tract and its impacts on oral delivery of nanoparticles.Med Res Rev. 2020 Dec 1. doi: 10.1002/med.21767. Online ahead of print. Med Res Rev. 2020. PMID: 33289146 Review.
-
Delivery of Orally Administered Digestible Antibodies Using Nanoparticles.Int J Mol Sci. 2021 Mar 25;22(7):3349. doi: 10.3390/ijms22073349. Int J Mol Sci. 2021. PMID: 33805888 Free PMC article. Review.
Cited by
-
The role of patient-specific variables in protein corona formation and therapeutic efficacy in nanomedicine.J Nanobiotechnology. 2024 Nov 15;22(1):714. doi: 10.1186/s12951-024-02954-y. J Nanobiotechnology. 2024. PMID: 39548452 Free PMC article. Review.
-
Inflammatory disease progression shapes nanoparticle biomolecular corona-mediated immune activation profiles.Nat Commun. 2025 Jan 22;16(1):924. doi: 10.1038/s41467-025-56210-4. Nat Commun. 2025. PMID: 39843415 Free PMC article.
-
Transepithelial transport of nanoparticles in oral drug delivery: From the perspective of surface and holistic property modulation.Acta Pharm Sin B. 2024 Sep;14(9):3876-3900. doi: 10.1016/j.apsb.2024.06.015. Epub 2024 Jun 22. Acta Pharm Sin B. 2024. PMID: 39309496 Free PMC article. Review.
References
-
- Okeyo P.O., Rajendran S.T., Zór K., Boisen A. Sensing technologies and experimental platforms for the characterization of advanced oral drug delivery systems. Adv Drug Deliv Rev. 2021;176 - PubMed
-
- Moss D.M., Curley P., Kinvig H., Hoskins C., Owen A. The biological challenges and pharmacological opportunities of orally administered nanomedicine delivery. Expet Rev Gastroenterol Hepatol. 2018;12:223–236. - PubMed
LinkOut - more resources
Full Text Sources
