

Glucometabolic outcomes of GLP-1 receptor agonist-based therapies in patients with type 2 diabetes: a systematic review and network meta-analysis
- PMID: 37719418
- PMCID: PMC10500557
- DOI: 10.1016/j.eclinm.2023.102181
Glucometabolic outcomes of GLP-1 receptor agonist-based therapies in patients with type 2 diabetes: a systematic review and network meta-analysis
Abstract
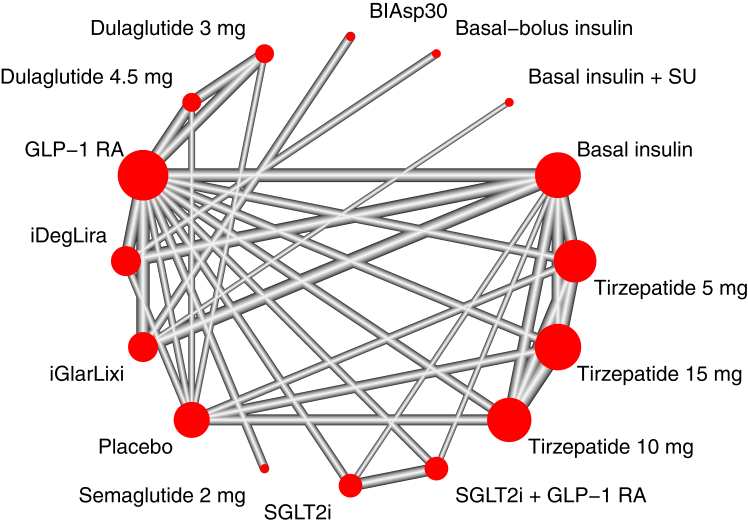
Background: Innovative GLP-1 receptor agonist (GLP-1RA)-based treatment strategies-such as tirzepatide, GLP-1RA plus basal insulin fixed-ratio combinations [FRC], GLP-1RA plus sodium glucose cotransporter-2 inhibitors [SGLT-2i] combinations, and high-dose GLP-1RA-have been listed among the most efficacious options for type 2 diabetes management. However, differences in their glucometabolic effects have not been assessed in dedicated head-to-head trials. In the absence of such trials, we aimed to provide a useful comparison among these treatment strategies to guide clinical practice.
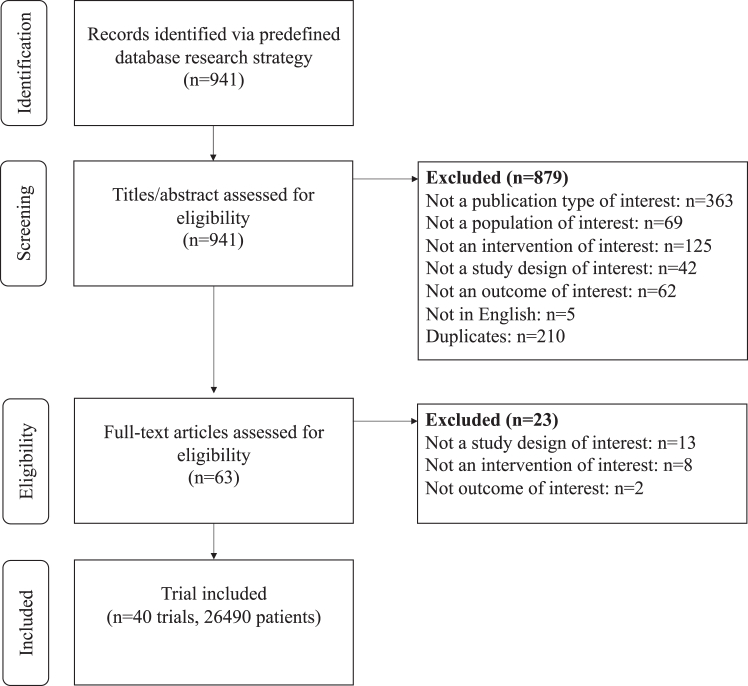
Methods: In this network meta-analysis, we searched PubMed, MEDLINE, and Web of Science (from database inception to June 24, 2023) for randomised controlled studies, published in English, that enrolled individuals with type 2 diabetes treated with tirzepatide, iGlarLixi, iDegLira, GLP-1RA plus SGLT-2i combination, or high-dose GLP-1RA (dulaglutide 3 mg and 4.5 mg, semaglutide 2 mg) compared with placebo or active comparators. Eligible studies reported change from baseline in HbA1c as an outcome, which was the primary outcome of this analysis. Secondary outcomes were changes in fasting and post-prandial glucose, bodyweight, LDL-cholesterol, blood pressure and risk of hypoglycaemia. We assessed risk of bias through the Cochrane Collaboration's tool (RoB2 tool), publication bias through visual inspection of funnel plots and Egger's test, and heterogeneity by comparing the magnitude of the common between-study variance (τ2) for each outcome with empirical distributions of heterogeneity variances. This network meta-analysis was registered in PROSPERO (CRD42022329878).
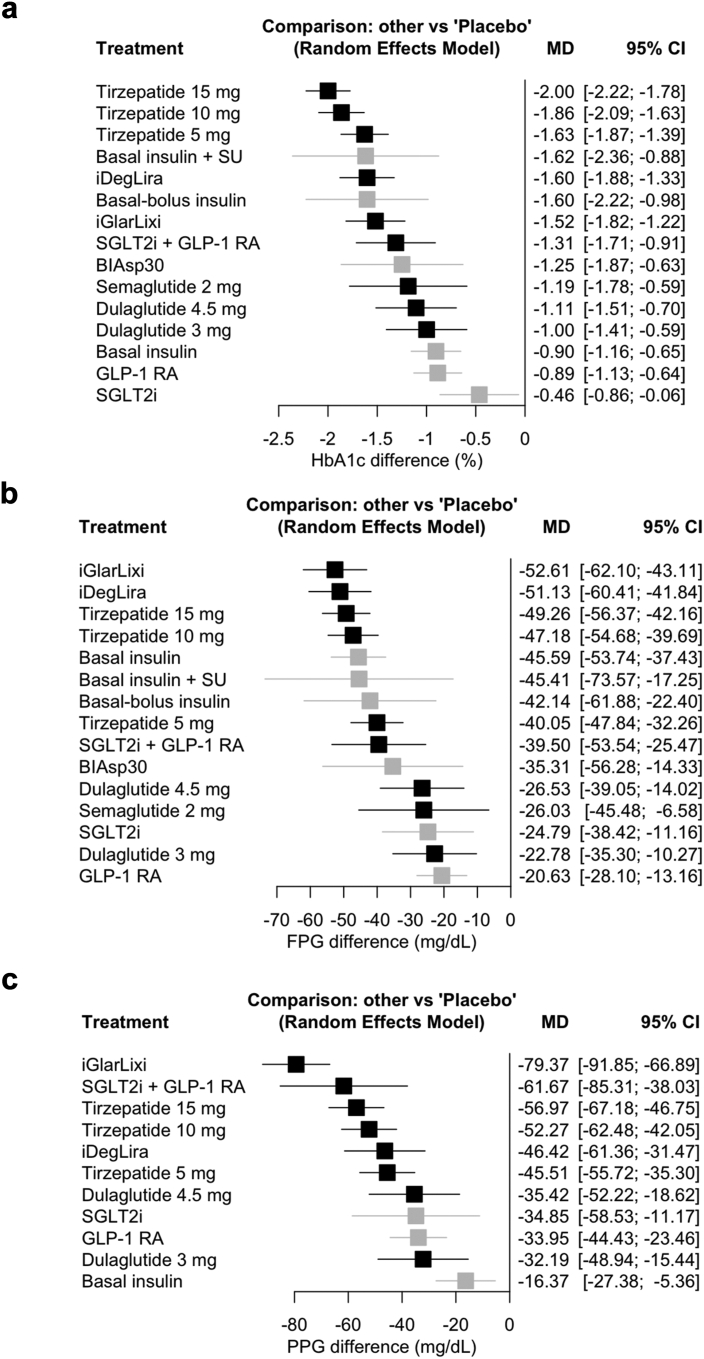
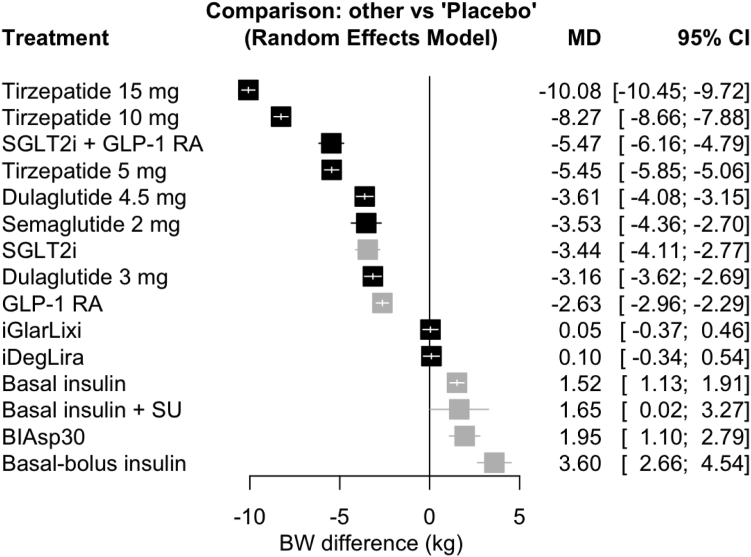
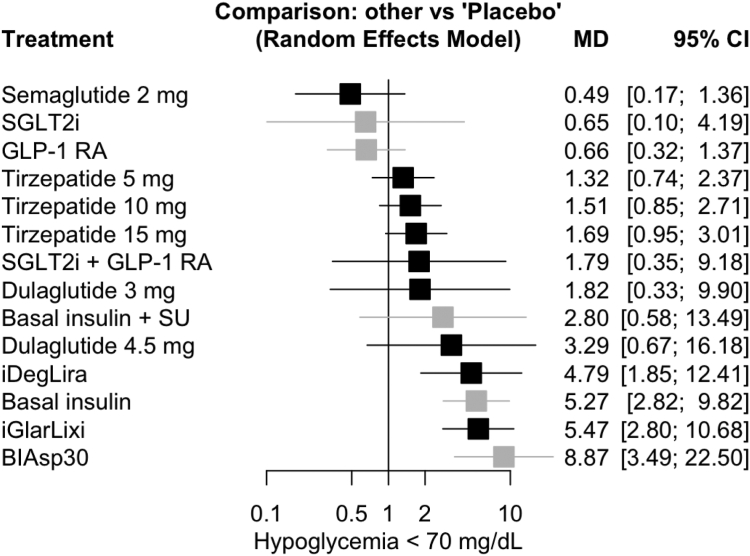
Findings: 40 trials were included. Tirzepatide 15 mg ranked first in terms of HbA1c reduction compared to other GLP-1RA-based strategies, even those including insulin (vs. iDegLira MD -0.40%, 95% CI [-0.66; -0.14], low certainty; vs. iGlarLixi MD -0.48%, 95% CI [-0.75; -0.21], low certainty), without increasing the risk of hypoglycaemia (vs. iDegLira OR 0.35, 95% CI [0.16; 0.79], high certainty; vs. iGlarLixi OR 0.31, 95% CI [0.20; 0.48], high certainty). Tirzepatide 15 mg was also the most efficacious on weight lowering, even compared to high-dose GLP-1RA (eg, semaglutide 2 mg MD -6.56 kg, 95% CI [-7.38; -5.73], low certainty) and GLP-1RA plus SGLT-2i combination (MD -4.61 kg, 95% CI [-5.29; -3.93], low certainty). Risk of bias and publication bias were generally low throughout studies, while high levels of heterogeneity were detected for most outcomes.
Interpretation: Aiming to support clinicians in tailoring treatment to patients' needs, we suggest that a hierarchy among treatment strategies be devised considering the best options for type 2 diabetes. Tirzepatide, followed by GLP-1RA plus basal insulin FRC and GLP-1RA plus SGLT-2i combination, was associated with greater benefit on HbA1c than high-dose GLP-1RA.
Funding: Fondazione per la Ricerca Biomedica "Saverio e Isabella Cianciola" and Next Generation EU, in the context of the National Recovery and Resilience Plan, Investment PE8-Project Age-It: Ageing Well in an Ageing Society.
Keywords: Fixed-ratio combination; GLP1-RA; Network meta-analysis; SGLT-2i; Tirzepatide.
© 2023 The Author(s).
Conflict of interest statement
AC reports the following: AstraZeneca, Eli Lilly, Novo Nordisk, Roche Diagnostics, Sanofi Aventis (honoraria). AN reports the following: AstraZeneca, Novo Nordisk, and Sanofi Aventis (honoraria). FG reports the following: Eli Lilly, Roche Diabetes Care (grants); Eli Lilly, Novo Nordisk (consulting fees); AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Lifescan, Merck Sharp & Dohme, Medtronic, Novo Nordisk, Roche Diabetes Care, Sanofi Aventis; Eli Lilly, Sanofi Aventis (support for attending meetings/travel); AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Lifescan, Merck Sharp & Dohme, Medimmune, Medtronic, Novo Nordisk, Roche Diabetes Care, Sanofi Aventis (participation on Advisory Boards); EASD/EFSD, Società Italiana di Endocrinologia (SIE), Fo.Ri.SIE (unpaid leadership); AstraZeneca, Eli Lilly, Novo Nordisk, Sanofi Aventis (support for medical writing and statistical analysis). GFMS: no competing interests. IC reports the following: Eli Lilly, Novo Nordisk (honoraria); Eli Lilly, Novo Nordisk (support for attending meeting or travels); LDG reports the following: Eli Lilly, MOVI SpA, Roche Diabetes Care (honoraria). LL reports the following: Abbott, AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Merck Sharp & Dohme, Medtronic, Menarini, MOVI SpA, Mundipharma, Novo Nordisk, Roche Diabetes Care, Sanofi Aventis, Terumo (honoraria); Abbott, AstraZeneca, Boeringher-Ingelheim, Eli Lilly Italia, Medtronic, MOVI SpA, Novo Nordisk, Roche Diabetes Care, Sanofi Aventis, Terumo (participation on Advisory Boards). PN: no competing interests. SDM reports the following: Ascensia, MOVI SpA, Roche Diabetes Care (honoraria); Ascensia, MOVI SpA, Roche Diabetes Care (participation on Advisory Boards). SCP: no competing interests. SP reports the following: AstraZeneca, Eli Lilly, Novo Nordisk, Sanofi Aventis (honoraria).
Figures
References
-
- Saeedi P., Petersohn I., Salpea P., et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9th edition. Diabetes Res Clin Pract. 2019;157 - PubMed
-
- Ussher J.R., Drucker D.J. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol. 2023;20:463–474. - PubMed
-
- De Block C.E.M., Dirinck E., Verhaegen A., Van Gaal L.F. Efficacy and safety of high-dose glucagon-like peptide-1, glucagon-like peptide-1/glucose-dependent insulinotropic peptide, and glucagon-like peptide-1/glucagon receptor agonists in type 2 diabetes. Diabetes Obes Metab. 2022;24:788–805. - PubMed
LinkOut - more resources
Full Text Sources
