

Visualization and clinical relevance of the endolymphatic duct and sac in Ménière's disease
- PMID: 37719762
- PMCID: PMC10501721
- DOI: 10.3389/fneur.2023.1239422
Visualization and clinical relevance of the endolymphatic duct and sac in Ménière's disease
Abstract
Background: Ménière's disease (MD) is a chronic inner ear disorder with a multifactorial etiology. Decreased visualization of the endolymphatic duct (ED) and sac (ES) is thought to be associated with MD, although controversy exists about whether this finding is specific to MD. Recent literature has revealed that two distinct ES pathologies, developmental hypoplasia and epithelial degeneration, can be distinguished in MD using the angular trajectory of the vestibular aqueduct (ATVA) or ED-ES system as a radiographic surrogate marker. It has been suggested that these two subtypes are associated with distinct phenotypical features. However, the clinical differences between the ATVA subtypes require further validation.
Research objective: The objective of this study is to investigate whether (1) non-visualization of the ED-ES system is a discriminative radiological feature for MD in a cohort of vertigo-associated pathologies (VAPs) and whether (2) different angular trajectories of the ED-ES system in MD are associated with distinguishable clinical features.
Setting: The study was conducted in the Vertigo Referral Center (Haga Teaching Hospital, The Hague, the Netherlands).
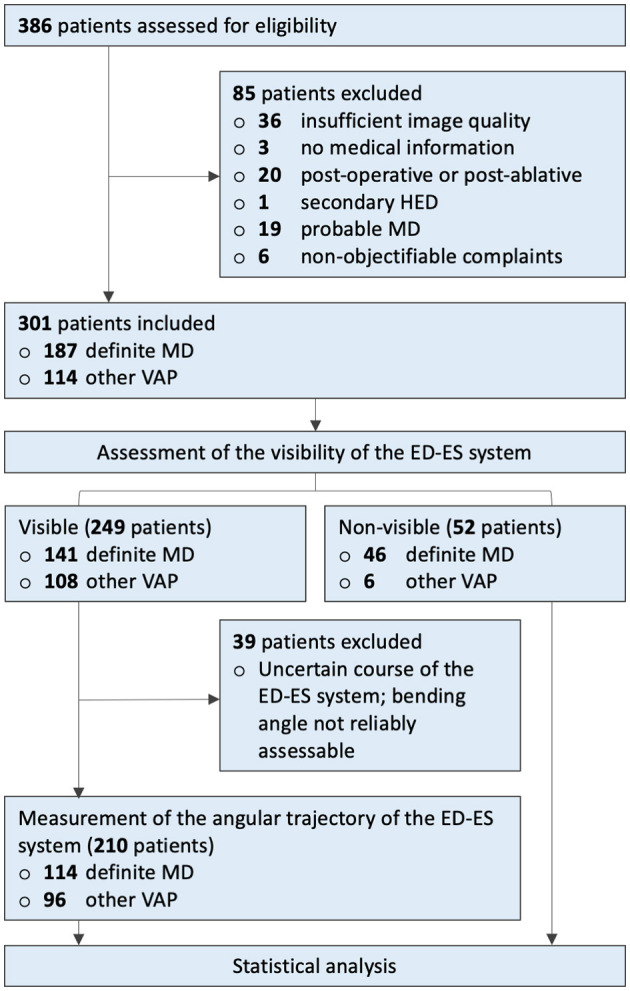
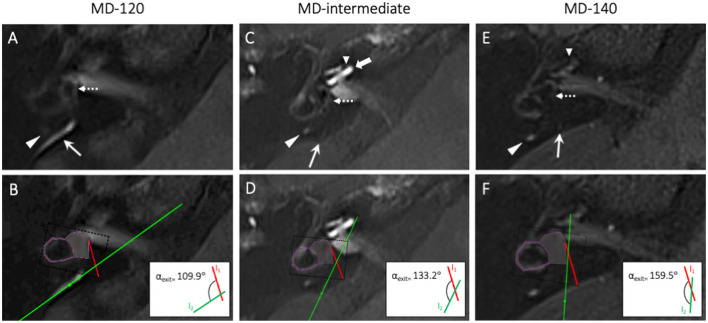
Methods: We retrospectively assessed 301 patients (187 definite MD and 114 other VAPs) that underwent 4h-delayed 3D FLAIR MRI. We evaluated (1) the visibility of the ED-ES system between MD and other VAP patients and (2) measured the angular trajectory of the ED-ES system. MD patients were stratified based on the angular measurements into αexit ≤ 120° (MD-120), αexit 120°-140° (MD-intermediate), or αexit ≥ 140° (MD-140). Correlations between ATVA subgroups and clinical parameters were evaluated.
Results: Non-visualization of the ED-ES system was more common in definite MD patients compared with other VAPs (P < 0.001). Among definite MD patients, the MD-140 subtype demonstrated a longer history of vertigo (P = 0.006), a higher prevalence of bilateral clinical disease (P = 0.005), and a trend toward a male preponderance (p = 0.053). No significant differences were found between ATVA subgroups regarding the presence or severity of auditory symptoms, or the frequency of vertigo attacks.
Conclusion: Non-visualization of the ED-ES system is significantly associated with MD. Among MD patients with a visible ED-ES system, we demonstrated that the MD-140 subtype is associated with a longer disease duration, a higher prevalence of bilateral MD, and a trend toward a male preponderance.
Keywords: MRI; Ménière; clinical features; endolymphatic duct; endolymphatic sac.
Copyright © 2023 de Pont, Houben, Verhagen, Verbist, Buchem, Bommeljé, Blom and Hammer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Angular Trajectory of the Vestibular Aqueduct in a Cohort of Chinese Patients with Unilateral Ménière's Disease: Association with Other Imaging Indices and Clinical Profiles.Biomedicines. 2024 Sep 3;12(9):2008. doi: 10.3390/biomedicines12092008. Biomedicines. 2024. PMID: 39335521 Free PMC article.
-
Vestibular Aqueduct Morphology Correlates With Endolymphatic Sac Pathologies in Menière's Disease-A Correlative Histology and Computed Tomography Study.Otol Neurotol. 2019 Jun;40(5):e548-e555. doi: 10.1097/MAO.0000000000002198. Otol Neurotol. 2019. PMID: 31083097 Free PMC article.
-
Contrast Agent Uptake in Endolymphatic Sac and Duct: Inverse Relation to Endolymphatic Hydrops.Laryngoscope. 2025 Aug;135(8):2914-2922. doi: 10.1002/lary.32127. Epub 2025 Mar 19. Laryngoscope. 2025. PMID: 40105260 Free PMC article.
-
Re-evaluation of the role of the human endolymphatic sac in Menière's disease.Otolaryngol Head Neck Surg. 1990 Jun;102(6):732-44. doi: 10.1177/019459989010200618. Otolaryngol Head Neck Surg. 1990. PMID: 2115662 Review.
-
Posterior petrous face meningiomas presenting with Ménière's-like syndrome: a case series and review of the literature.J Neurosurg. 2021 Aug 27;136(2):441-448. doi: 10.3171/2021.2.JNS203259. Print 2022 Feb 1. J Neurosurg. 2021. PMID: 34450586 Review.
Cited by
-
Comparison of vestibular aqueduct visualization on computed tomography and magnetic resonance imaging in patients with Ménière's disease.BMC Med Imaging. 2024 Apr 22;24(1):93. doi: 10.1186/s12880-024-01275-8. BMC Med Imaging. 2024. PMID: 38649991 Free PMC article.
-
Dual-target corticosteroid therapy for refractory Ménière's disease: influence of vestibular aqueduct patency and endotypes.Eur Arch Otorhinolaryngol. 2025 Jul 4. doi: 10.1007/s00405-025-09542-2. Online ahead of print. Eur Arch Otorhinolaryngol. 2025. PMID: 40615707 No abstract available.
-
Retrolabyrinthine Bone Thickness as a Radiologic Marker for the Hypoplastic Endotype in Menière Disease.AJNR Am J Neuroradiol. 2024 Sep 9;45(9):1363-1369. doi: 10.3174/ajnr.A8339. AJNR Am J Neuroradiol. 2024. PMID: 39054294
-
Angular Trajectory of the Vestibular Aqueduct in a Cohort of Chinese Patients with Unilateral Ménière's Disease: Association with Other Imaging Indices and Clinical Profiles.Biomedicines. 2024 Sep 3;12(9):2008. doi: 10.3390/biomedicines12092008. Biomedicines. 2024. PMID: 39335521 Free PMC article.
-
Vestibular Aqueduct and Temporal Bone Radioanatomy in Patients With and Without Meniere Disease: A Retrospective Cross-Sectional Analysis With Implications for Endolymphatic Sac Surgery.Clin Exp Otorhinolaryngol. 2025 May;18(2):162-170. doi: 10.21053/ceo.2024.00334. Epub 2025 Mar 24. Clin Exp Otorhinolaryngol. 2025. PMID: 40127501 Free PMC article.
References
LinkOut - more resources
Full Text Sources