

Clinical relevance of salivary pepsin detection in diagnosing gastroesophageal reflux disease subtypes
- PMID: 37720194
- PMCID: PMC10500079
- DOI: 10.1093/gastro/goad053
Clinical relevance of salivary pepsin detection in diagnosing gastroesophageal reflux disease subtypes
Abstract
Background: Gastroesophageal reflux disease (GERD) is heterogeneous with a varied symptom spectrum and reflux profiles. Its definite diagnosis often requires invasive tools including endoscopy or reflux monitoring. The aim of this study was to investigate the clinical relevance of salivary pepsin detection as a non-invasive screening tool to diagnose GERD of different subtypes.
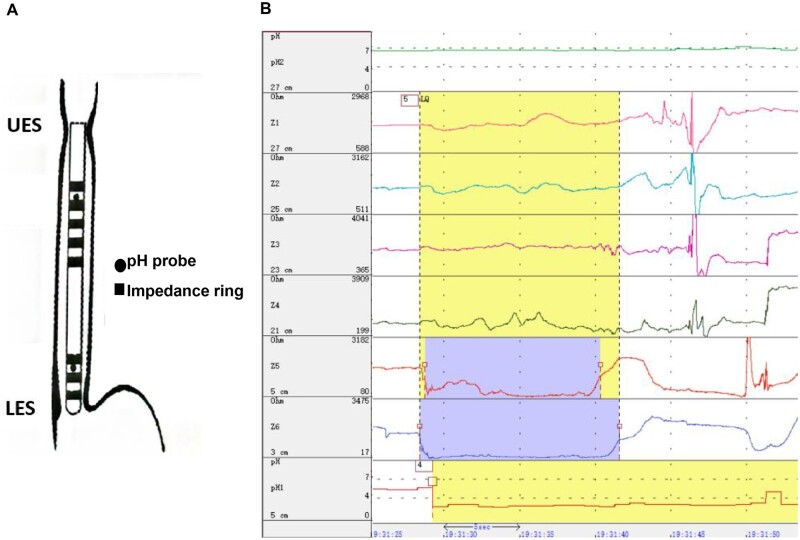
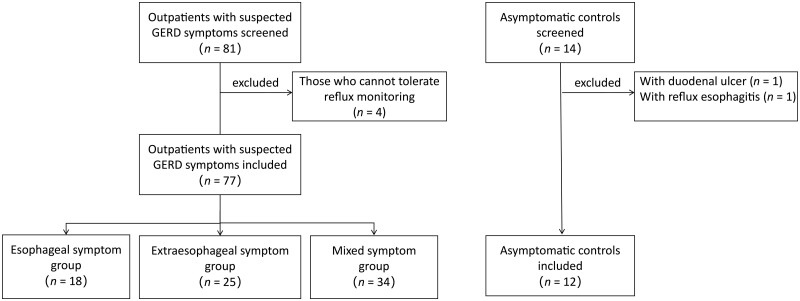
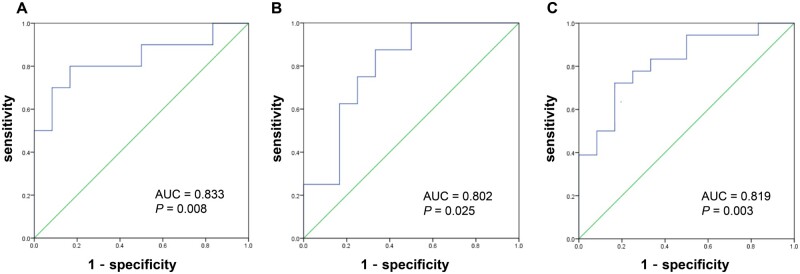
Methods: A total of 77 patients with suspected GERD symptoms and 12 asymptomatic controls were analysed. All participants performed symptom evaluation, upper endoscopy, esophageal manometry, and 24-hour multichannel intraluminal impedance-dual pH probe monitoring. Saliva was self-collected across three different time points: at early fasting, postprandially, and at symptom occurrence. Salivary pepsin levels were measured via Peptest. The optimal threshold of salivary pepsin for diagnosing distal or proximal reflux was determined according to a receiver-operating characteristic curve.
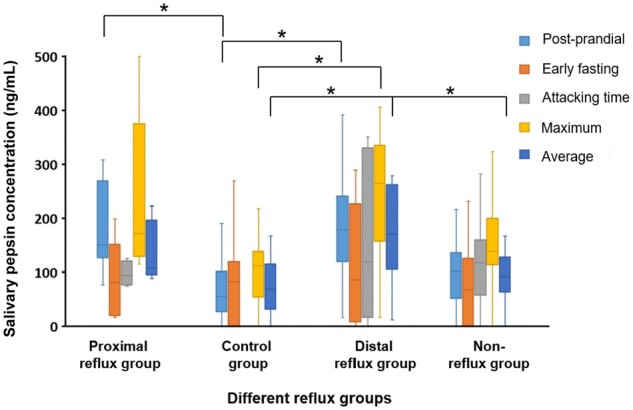
Results: The average salivary pepsin concentration of suspected GERD patients was significantly higher than that of controls (100.63 [68.46, 141.38] vs 67.90 [31.60, 115.06] ng/mL, P = 0.044), although no difference was found among patients with different symptom spectrums. The distal reflux group had a higher average pepsin concentration than non-reflux patients (170.54 [106.31, 262.76] vs 91.13 [63.35, 127.63] ng/mL, P = 0.043), while no difference was observed between the distal reflux group and the proximal reflux group. The optimal cut-off value of salivary pepsin concentration for diagnosing pathological distal reflux was 157.10 ng/mL, which was higher than that for diagnosing pathological proximal reflux (122.65 ng/mL). The salivary pepsin concentration was significantly correlated with distal and proximal reflux parameters.
Conclusions: Salivary pepsin measurement can help in identifying true GERD with pathological distal reflux or proximal reflux, regardless of different symptom spectrums. A higher threshold should be applied for diagnosing distal reflux than for proximal reflux.
Keywords: gastroesophageal reflux disease; laryngopharyngeal reflux; salivary pepsin; screening and diagnosis.
© The Author(s) 2023. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Pathogenesis of pepsin-induced gastroesophageal reflux disease with advanced diagnostic tools and therapeutic implications.Front Med (Lausanne). 2025 Feb 19;12:1516335. doi: 10.3389/fmed.2025.1516335. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40046936 Free PMC article. Review.
-
The Role of Salivary Pepsin in the Diagnosis of Gastroesophageal Reflux Disease (GERD) Evaluated Using High-Resolution Manometry and 24-Hour Multichannel Intraluminal Impedance-pH Monitoring.Med Sci Monit. 2020 Nov 21;26:e927381. doi: 10.12659/MSM.927381. Med Sci Monit. 2020. PMID: 33220027 Free PMC article.
-
Gastroesophageal reflux disease and salivary pepsin in patients with heterotopic gastric mucosa in the upper esophagus.Dis Esophagus. 2022 Apr 19;35(4):doab074. doi: 10.1093/dote/doab074. Dis Esophagus. 2022. PMID: 34750620
-
The diagnostic value of pepsin detection in saliva for gastro-esophageal reflux disease: a preliminary study from China.BMC Gastroenterol. 2017 Oct 17;17(1):107. doi: 10.1186/s12876-017-0667-9. BMC Gastroenterol. 2017. PMID: 29041918 Free PMC article.
-
Salivary peptest for laryngopharyngeal reflux and gastroesophageal reflux disease: A systemic review and meta-analysis.Medicine (Baltimore). 2021 Aug 13;100(32):e26756. doi: 10.1097/MD.0000000000026756. Medicine (Baltimore). 2021. PMID: 34397878 Free PMC article.
Cited by
-
Pathogenesis of pepsin-induced gastroesophageal reflux disease with advanced diagnostic tools and therapeutic implications.Front Med (Lausanne). 2025 Feb 19;12:1516335. doi: 10.3389/fmed.2025.1516335. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40046936 Free PMC article. Review.
References
-
- Eusebi LH, Ratnakumaran R, Yuan Y. et al. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 2018;67:430–40. - PubMed
-
- Xiao YL, Zhou LY, Hou XH. et al.; Chinese Society of Gastroenterology. Chinese expert consensus on gastroesophageal reflux disease in 2020. J Dig Dis 2021;22:376–89. - PubMed
-
- Savarino E, Zentilin P, Savarino V.. NERD: an umbrella term including heterogeneous subpopulations. Nat Rev Gastroenterol Hepatol 2013;10:371–80. - PubMed
-
- Barrett CM, Patel D, Vaezi MF.. Laryngopharyngeal reflux and atypical gastroesophageal reflux disease. Gastrointest Endosc Clin N Am 2020;30:361–76. - PubMed
LinkOut - more resources
Full Text Sources
