

Protective effect of hydroxychloroquine on infections in patients with systemic lupus erythematosus: an observational study using the LUNA registry
- PMID: 37720209
- PMCID: PMC10504661
- DOI: 10.3389/fimmu.2023.1227403
Protective effect of hydroxychloroquine on infections in patients with systemic lupus erythematosus: an observational study using the LUNA registry
Abstract
Objectives: Infection is a leading cause of death in patients with systemic lupus erythematosus (SLE). Alt hough hydroxychloroquine (HCQ) has been reported to inhibit infection, evidence from Asian populations remains insufficient. We investigated this effect in Japanese SLE patients.
Methods: Data from the Lupus Registry of Nationwide Institutions were used in this study. The patients were ≥20 years old and met the American College of Rheumatology (ACR) classification criteria revised in 1997. We defined "severe infections" as those requiring hospitalization. We analyzed the HCQ's effect on infection suppression using a generalized estimating equation (GEE) logistic regression model as the primary endpoint and performed a survival analysis for the duration until the first severe infection.
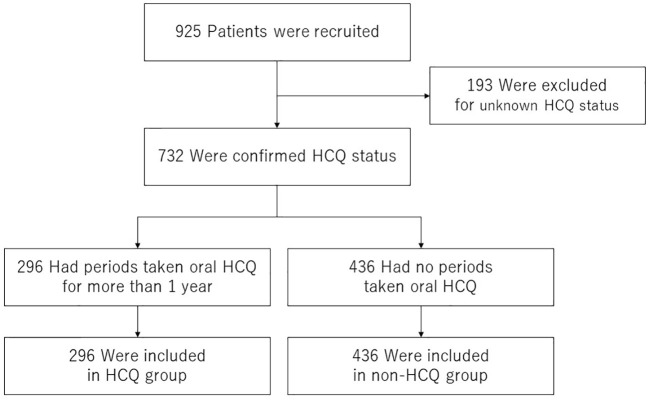
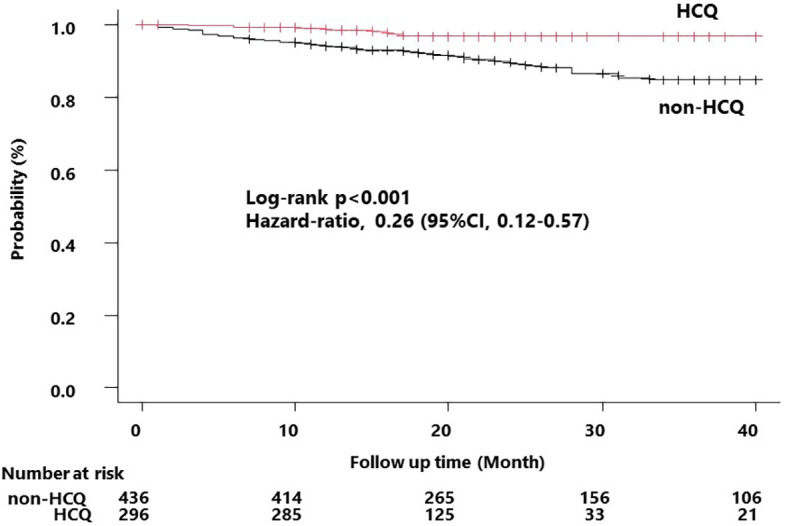
Results: Data from 925 patients were used (median age, 45 [interquartile range 35-57] years; female, 88.1%). GEE analysis revealed that severe infections were significantly associated with glucocorticoid dose (odds ratio [OR] 1.968 [95% confidence interval, 1.379-2.810], p<0.001), immunosuppressants (OR 1.561 [1.025-2.380], p=0.038), and baseline age (OR 1.043 [1.027-1.060], p<0.001). HCQ tended to suppress severe infections, although not significantly (OR 0.590 [0.329-1.058], p=0.077). Survival time analysis revealed a lower incidence of severe infections in the HCQ group than in the non-HCQ group (p<0.001). In a Cox proportional hazards model, baseline age (hazard ratio [HR] 1.029 [1.009-1.050], p=0.005) and HCQ (HR 0.322 [0.142-0.728], p=0.006) were significantly related to incidence.
Conclusion: HCQ may help extend the time until the occurrence of infection complications and tends to decrease infection rates.
Keywords: Asian; hydroxychloroquine; infection; multicenter registry; systemic lupus erythematosus (SLE).
Copyright © 2023 Hidekawa, Yoshimi, Saigusa, Tamura, Kojitani, Suzuki, Sakurai, Yoshioka, Sugiyama-Kawahara, Kunishita, Kishimoto, Higashitani, Sato, Komiya, Nagai, Hamada, Maeda, Tsuchida, Hirahara, Soejima, Takase-Minegishi, Kirino, Yajima, Sada, Miyawaki, Ichinose, Ohno, Kajiyama, Sato, Shimojima, Fujiwara and Nakajima.
Conflict of interest statement
KS received a speaker’s fee from GlaxoSmithKline PLC and research grants from Pfizer Inc. YKi received a speaker’s fee from Amgen and Novartis and research funding from Nippon Shinyaku. RY received a speaker’s fee from GlaxoSmithKline PLC, AstraZeneca PLC, and Sanofi S.A. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous