

The impact of EMA recommendations on the real-life use of Janus kinases inhibitors for rheumatoid arthritis: the Expanded Risk Score in RA as a tool to quantify the risk of cardiovascular events
- PMID: 37720218
- PMCID: PMC10500057
- DOI: 10.3389/fimmu.2023.1225160
The impact of EMA recommendations on the real-life use of Janus kinases inhibitors for rheumatoid arthritis: the Expanded Risk Score in RA as a tool to quantify the risk of cardiovascular events
Abstract
Objective: To evaluate in patients with rheumatoid arthritis (RA) the impact of EMA recommendations on the real-life prescription of JAK inhibitors (JAKis) and the use of the Expanded Risk Score in RA (ERS-RA) to quantify the risk of major adverse cardiac events (MACE).
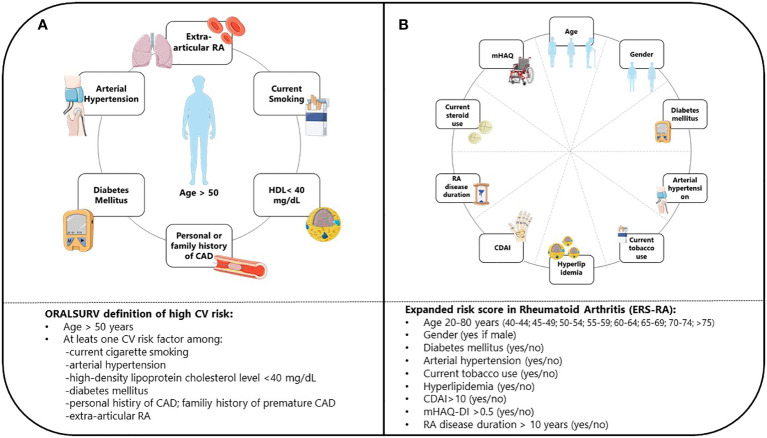
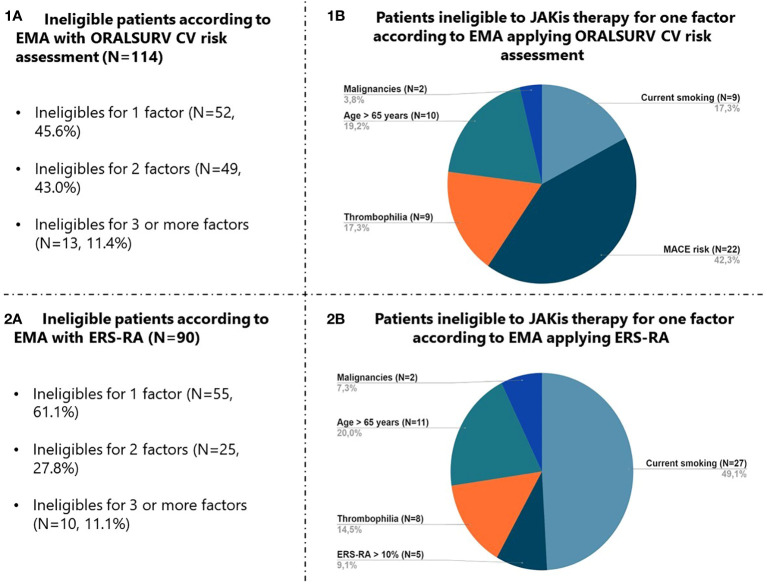
Methods: We conducted a retrospective analysis of real-life RA patients treated with JAKis. Patients were classified as ineligible for JAKis if they fulfilled EMA criteria (>65 years-old, history of malignancy, or increased risk of venous thromboembolic events [VTE] or MACE including smoking). Risk of MACE was defined according to ORAL Surveillance trial inclusion criteria (ORALSURV) or by using the ERS-RA.
Results: Of 194 patients enrolled, 57.9% were classified as ineligible according to EMA definition (ORALSURV criteria). The most frequent reason for ineligibility was increased MACE risk (70.2%), followed by age>65 (34.2%), smoking (30.7%), and increased risk of VTE (20.2%) or malignancy (7%). The use of the ERS-RA reduced the rate of patients carrying an increased CV risk to 18.6% (p<0.001 versus ORALSURV), leading to 46.4% overall ineligible patients. Over a drug-exposure of 337 patient/years, we observed 2 VTE, one MACE (non-fatal stroke), and one solid malignancy (all in the group of patients classified as ineligible according to both the definitions).
Conclusions: Rigorous application of EMA indications in clinical practice could result in the exclusion of a large proportion of RA patients from treatment with JAKis. A proper quantification of the risk for MACE by dedicated tools as ERS-RA is advocated to better tailor the management of RA.
Keywords: JAK inhibitors; b/tsDMARDs; cardiovascular risk; rheumatoid arthritis; safety.
Copyright © 2023 Favalli, Cincinelli, Germinario, Di Taranto, Orsini, Maioli, Biggioggero, Ferrito and Caporali.
Conflict of interest statement
Author EF has been a consultant for and/or received honoraria as a speaker for the companies AbbVie, BMS, Eli Lilly, Galapagos, Janssen, MSD, Novartis, Pfizer, and UCB Pharma. Author MB received honoraria as a speaker for the company Galapagos. Author RC has been a consultant for and/or received honoraria as a speaker for the companies AbbVie, Amgen, BMS, Celltrion, Fresenius, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB Pharma. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials