

Metastatic well differentiated serotonin-producing pancreatic neuroendocrine tumor with carcinoid heart disease: a case report
- PMID: 37720425
- PMCID: PMC10502540
- DOI: 10.21037/jgo-22-909
Metastatic well differentiated serotonin-producing pancreatic neuroendocrine tumor with carcinoid heart disease: a case report
Abstract
Background: Less than two percent of pancreatic neuroendocrine tumors (NETs) produce serotonin. Serotonin can cause carcinoid syndrome and less commonly carcinoid heart disease (CHD). CHD is associated with increased mortality and requires a more aggressive approach. Here we present a rare case of a serotonin-producing pancreatic NET complicated by CHD at presentation and discuss timing of systemic therapy, liver-directed therapy, and heart failure management.
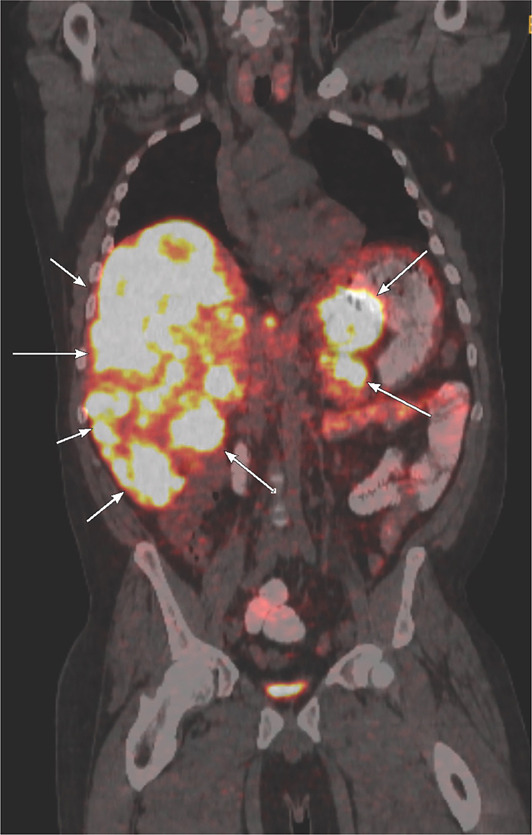
Case description: A 36-year-old white man presented with diarrhea, lower extremity edema, and exertional dyspnea. He was found to have a well-differentiated serotonin-producing pancreatic NETs grade three with bilobar liver metastasis complicated by carcinoid syndrome and CHD. His symptoms and disease burden improved with somatostatin analog and liver-directed therapy with bland embolization to control carcinoid symptoms and obtain rapid hormonal control to prevent progression of CHD. He concurrently received diuretics to manage his heart failure and was considered for valvular replacement surgery, which was deferred for optimal hormonal control.
Conclusions: Our case highlights the importance of multidisciplinary care for patients with pancreatic NETs and early identification and management of CHD. Although uncommon, serotonin-producing pancreatic NETs can present with CHD and require combination of somatostatin analogs, liver-directed therapy, and heart failure management.
Keywords: Case report; carcinoid; carcinoid heart disease (CHD); neuroendocrine tumor (NET); pancreatic NET (PaNET).
2023 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-22-909/coif). The series “Educational Case Series of the Memorial Sloan Kettering Cancer Center” was commissioned by the editorial office without any funding or sponsorship. GKA served as the unpaid Guest Editor for the series and he received research support from Arcus, Agios, Astra Zeneca, BioNtech, BMS, Celgene, Flatiron, Genentech/Roche, Genoscience, Incyte, Polaris, Puma, QED, Silenseed, Yiviva, and consulting support for efforts with Adicet, Astra Zeneca, Alnylam, Autem, Bayer, Beigene, Berry Genomics, Cend, Celgene, CytomX, Eisai, Eli Lilly, Exelixis, Flatiron, Genentech/Roche, Genoscience, Helio, Incyte, Ipsen, Legend Biotech, Merck, Nerviano, QED, Redhill, Rafael, Servier, Silenseed, Sillajen, Sobi, Surface Oncology, Therabionics, Vector, and Yiviva. EOR declares research funding to Institution from Genentech/Roche, Celgene/BMS, BioNTech, AstraZeneca, Arcus, Elicio, Parker Institute, American Association of Cancer Research, Imedex and Shanghai Jo’Ann Medical Technology Co., Ltd, consulting fees from Seagen, Boehringer Ingelheim, BioNTech, Ipsen, Merck, IDEAYA, Silenseed, Novartis, AstraZeneca, Noxxon, BioSapien, Cend Therapeutics, Astellas, Thetis, Autem, ZielBio, Tempus, Research To Practice, Agios (spouse), Genentech-Roche (spouse), Eisai (spouse), and she is on Data Safety Monitoring Board of Cytomx Therapeutics (DSMB) and Rafael Therapeutics (DSMB). BS declares unpaid memberships on committees for Lancet Oncology international advisory board, UK global cancer network steering committee, ASCO, Cansupport management committee, EBMT nuclear accident committee and ISMP executive committee. KG reports grants from NIH/NCI, AACR, Burroughs Wellcome Funds, Damon Runyon Cancer Research Foundation, Pershing Square Sohn Foundation, Stand Up to Cancer, Josie Robertson Foundation, Anna fuller foundation, Dalton Family Foundation. The authors have no other conflict of interest to report.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases