

Rifampin Based Therapy for Patients With Staphylococcus aureus Native Vertebral Osteomyelitis: A Systematic Review and Meta-analysis
- PMID: 37721158
- PMCID: PMC11487109
- DOI: 10.1093/cid/ciad560
Rifampin Based Therapy for Patients With Staphylococcus aureus Native Vertebral Osteomyelitis: A Systematic Review and Meta-analysis
Abstract
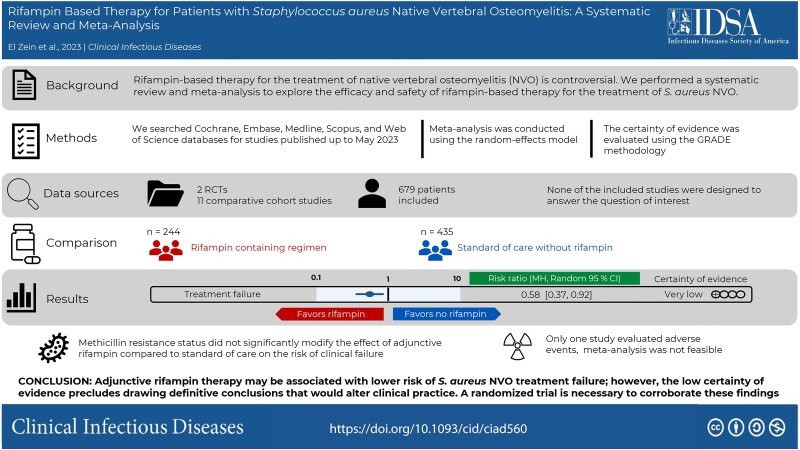
Background: Native vertebral osteomyelitis (NVO) caused by Staphylococcus aureus is associated with high risk of treatment failure and increased morbidity. The role of rifampin-based therapy for the treatment of this condition is controversial. The goal of this systematic review and meta-analysis is to explore the efficacy and safety of rifampin-based therapy for the treatment of S. aureus NVO.
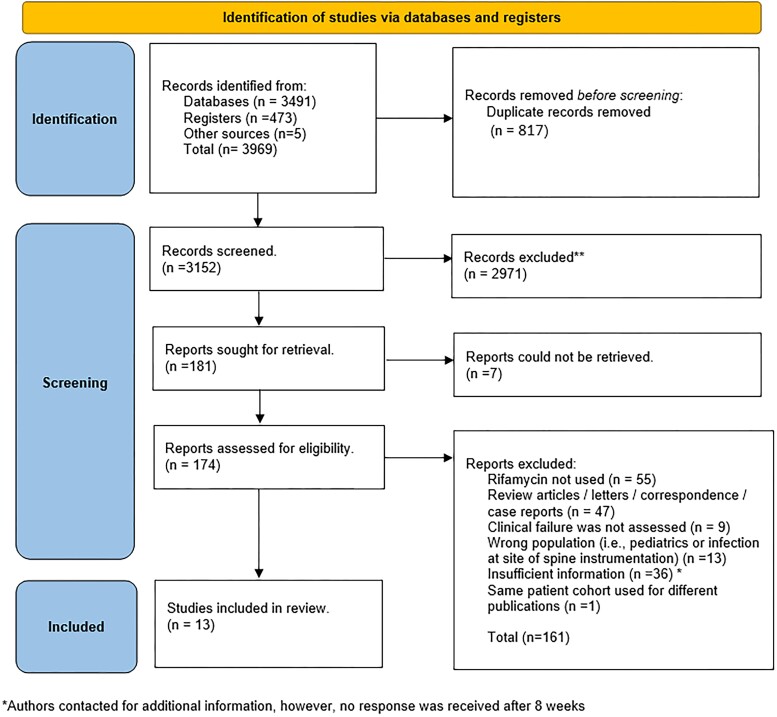
Methods: We searched Cochrane, Embase, Medline, Scopus, and Web of Science databases for studies published up to May 2023, focusing on adults with NVO treated with or without rifampin-containing regimens. A random-effects model meta-analysis estimated relative risks and risk difference with 95% confidence intervals (CI).
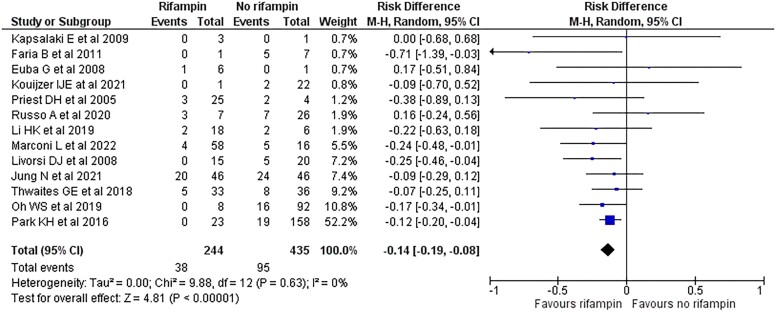
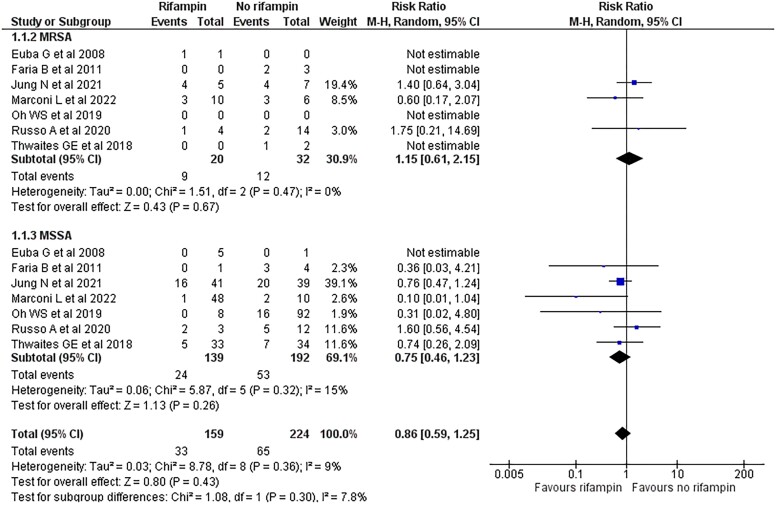
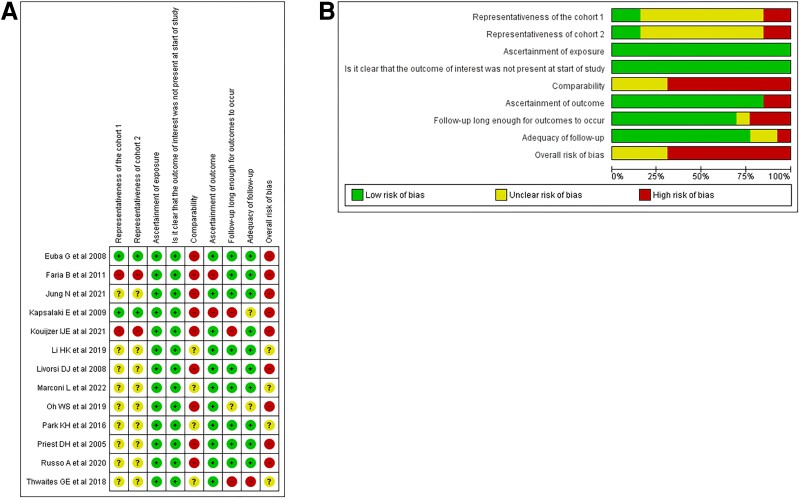
Results: Thirteen studies (2 randomized controlled trials and 11 comparative cohort studies), comprising 244 patients with S. aureus NVO who received rifampin and 435 who did not, were analyzed. Meta-analysis showed that rifampin-based regimens were associated with lower risk of clinical failure (risk difference, -14%; 95% CI, -19% to -8%; P < .001; I2 = 0%; relative risk, 0.58; 95% CI, .37-.92, P = .02, I2 = 21%). Only 1 study reported on adverse events. All studies had a high or uncertain risk of bias, and the certainty of evidence was rated as very low.
Conclusions: Adjunctive rifampin therapy might be associated with lower risk of S. aureus NVO treatment failure; however, the low certainty of evidence precludes drawing definitive conclusions that would alter clinical practice. A randomized trial is necessary to corroborate these findings.
Keywords: NVO; native vertebral osteomyelitis; rifampicin; rifampin; spondylodiscitis.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. S. E. Z, E. F. B. , M. P., F. P., J. M., M. H. M., P. S., and A. J. T. declare no competing interests. A. J. T. reports honoraria for medical writing from UpToDate; a role as unpaid executive board member for Musculoskeletal Infection Society. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Issa K, Diebo BG, Faloon M, et al. The epidemiology of vertebral osteomyelitis in the United States from 1998 to 2013. Clin Spine Surg 2018; 31:E102–8. - PubMed
-
- Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A. Pyogenic vertebral osteomyelitis: a systematic review of clinical characteristics. Semin Arthritis Rheum 2009; 39:10–7. - PubMed
-
- Park K-HC, Hyun O, Lee J-H, et al. Optimal duration of antibiotic therapy in patients with hematogenous vertebral osteomyelitis at low risk and high risk of recurrence. Clin Infect Dis 2016; 62:1262–9. - PubMed
