

Oncological recurrence following pathological complete response after neoadjuvant treatment in patients with esophageal cancer - a retrospective cohort study
- PMID: 37721586
- PMCID: PMC10506930
- DOI: 10.1007/s00423-023-03100-2
Oncological recurrence following pathological complete response after neoadjuvant treatment in patients with esophageal cancer - a retrospective cohort study
Abstract
Background: To evaluate recurrence in patients with post-neoadjuvant pathological complete response (pCR) and in patients with complete response of primary tumor but persisting lymphatic spread of disease (non-pCR, ypT0ypN +) of esophageal cancer.
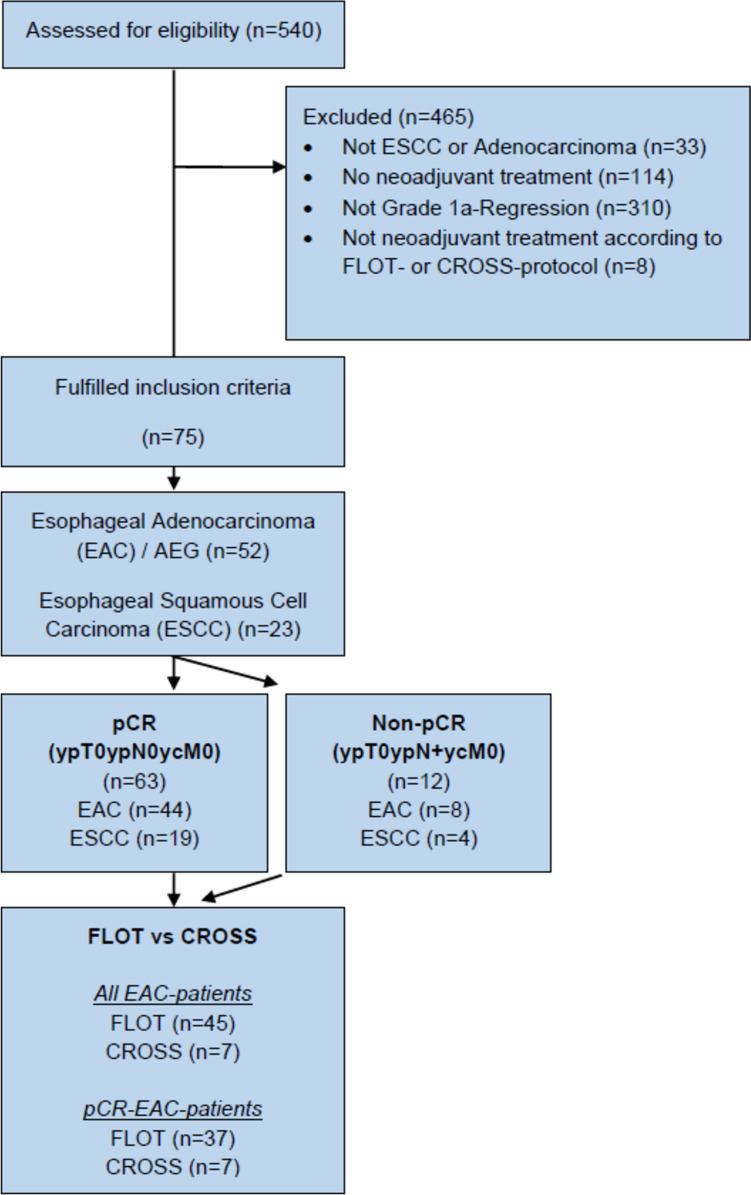
Methods: Seventy-five patients (63 pCR, 12 non-pCR) were analyzed retrospectively. Pattern and incidence of local and distant recurrence as well as the impact on overall (OS) and disease-free survival (DFS) were evaluated. The efficacy of neoadjuvant chemotherapy according to FLOT protocol was compared to neoadjuvant chemoradiation according to CROSS protocol.
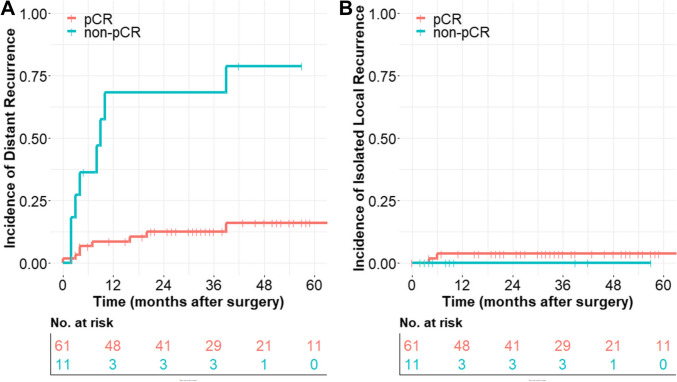
Results: In the pCR group, isolated local recurrence was diagnosed in 3%, while no isolated local recurrence was observed in the non-pCR group due to the high incidence of distant recurrence. Distant recurrence was most common in both cohorts (isolated distant recurrence: pCR group 10% to non-pCR group 55%; simultaneous distant and local recurrence: pCR group 3% to non-pCR group 18%). Median time to distant recurrence was 5.5 months, and median time to local recurrence was 8.0 months. Cumulative incidence of distant recurrence (with and without simultaneous local recurrence) was 16% (± 6%) in pCR patients and 79% (± 13%) in non-pCR patients (hazard ratio (HR) 0.123) estimated by Kaplan-Meier method. OS (HR 0.231) and DFS (HR 0.226) were significantly improved in patients with pCR compared to patients with non-pCR. Advantages for FLOT protocol compared to CROSS protocol, especially with regard to distant control of disease (HR 0.278), were observed (OS (HR 0.361), DFS (HR 0.226)).
Conclusion: Distant recurrence is the predominant site of treatment failure in patients with pCR and non-pCR grade 1a regression, whereby recurrence rates are much higher in patients with non-pCR.
Keywords: Chemoradiation; Chemotherapy; Esophageal cancer; Esophagogastric junction cancer; Multimodal treatment; Neoadjuvant treatment; Oncologic surgery; Pathological complete response; Visceral surgery.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven HWM, Nieuwenhuijzen GAP, Hospers GAP, Bonenkamp JJ, Cuesta MA, Blaisse RJB, Busch ORC, Ten Kate FJW, Creemers GM, Punt CJA, Plukker JTM, Verheul HMW, Bilgen EJS, van Dekken H, Van der Sangen MJC, Rozema T, Biermann K, Beukema JC, Piet AHM, van Rij CM, Reinders JG, Tilanus HW, Steyerberg EW, Van der Gaast A. CROSS study group Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer. (CROSS) long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–1098. doi: 10.1016/S1470-2045. - DOI - PubMed
-
- Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, Kopp HG, Mayer F, Haag GM, Luley K, Lindig U, Schmiegel W, Pohl M, Stoehlmacher J, Folprecht G, Probst S, Prasnikar N, Fischbach W, Mahlberg R, Trojan J, Koenigsmann M, Martens UM, Thuss-Patience P, Egger M, Block A, Heinemann V, Illerhaus G, Moehler M, Schenk M, Kullmann F, Behringer DM, Heike M, Pink D, Teschendorf C, Löhr C, Bernhard H, Schuch G, Rethwisch V, von Weikersthal LF, Hartmann JT, Kneba M, Daum S, Schulmann K, Weniger J, Belle S, Gaiser T, Oduncu FS, Güntner M, Hozaeel W, Reichart A, Jäger E, Kraus T, Mönig S, Bechstein WO, Schuler M, Schmalenberg H, Hofheinz RD. FLOT4-AIO Investigators. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948–1957. doi: 10.1016/S0140-6736(18)32557-1. - DOI - PubMed
-
- Blum Murphy M, Xiao L, Patel VR, DM Maru, Correa AM G, Amlashi F, Liao Z, Komaki R, Lin SH, Skinner HD, Vaporciyan A, Gl Walsh, Swisher SG, Sepesi B, Lee JH, Ms Bhutani, Weston B, Hofstetter WL, Ja Ajani. Pathological complete response in patients with esophageal cancer after the trimodality approach: the association with baseline variables and survival-The University of Texas MD Anderson Cancer Center experience. Cancer. 2017;123(21):4106–4113. doi: 10.1002/cncr.30953. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
