

Differences between cardiogenic shock related to acute decompensated heart failure and acute myocardial infarction
- PMID: 37723131
- PMCID: PMC10682868
- DOI: 10.1002/ehf2.14510
Differences between cardiogenic shock related to acute decompensated heart failure and acute myocardial infarction
Abstract
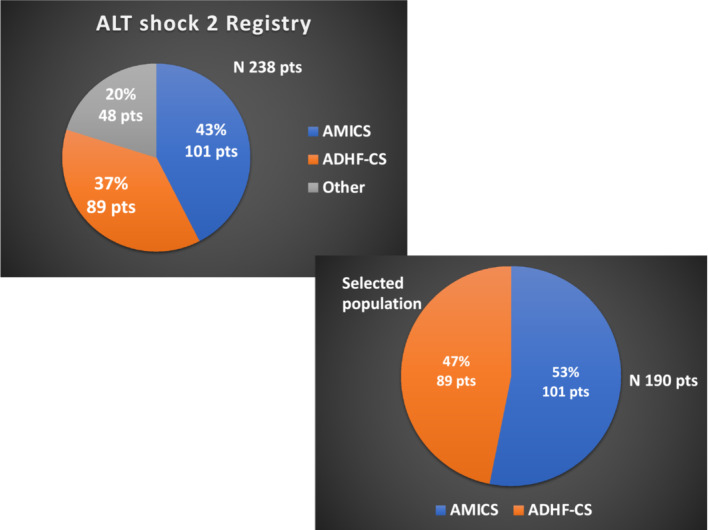
Aims: The present analysis from the multicentre prospective Altshock-2 registry aims to better define clinical features, in-hospital course, and management of cardiogenic shock complicating acutely decompensated heart failure (ADHF-CS) as compared with that complicating acute myocardial infarction (AMI-CS).
Methods and results: All patients with AMI-CS or ADHF-CS enrolled in the Altshock-2 registry between March 2020 and February 2022 were selected. The primary objective was the characterization of ADHF-CS patients as compared with AMI-CS. In-hospital length of stay and mortality were secondary endpoints. One-hundred-ninety of the 238 CS patients enrolled in the aforementioned period were considered for the present analysis: 101 AMI-CS (80% ST-elevated myocardial infarction and 20% non-ST-elevated myocardial infarction) and 89 ADHF-CS. As compared with AMI-CS, ADHF-CS patients were younger [63 (IQR 59-76) vs. 67 (IQR 54-73) years, P = 0.01], but presented with higher creatinine [1.6 (IQR 1.0-2.6) vs. 1.2 (IQR 1.0-1.4) mg/dL, P < 0.001], bilirubin [1.3 (IQR 0.9-2.3) vs. 0.6 (IQR 0.4-1.1) mg/dL, P = 0.01], and central venous pressure values [14 mmHg (IQR 8-12) vs. 10 mmHg (IQR 7-14),P = 0.01]. Norepinephrine was the most common catecholamine used in AMI-CS (79.3%), whereas epinephrine was used more commonly in ADHF-CS (65.5%); 75.8% vs. 46.6% received a temporary mechanical support in AMI-CS and ADHF-CS, respectively (P < 0.001). Length of hospital stay was longer in the latter [28 (IQR 13-48) vs. 17 (IQR 9-29) days, P = 0.001]. Heart replacement therapies were more frequently used in the ADHF-CS group (heart transplantation 13.5% vs. 0% and left ventricular assist device 11% vs. 2%, P < 0.01 and 0.01, respectively). In-hospital mortality was 41.1% (38.6% AMI-CS vs. 43.8% ADHF-CS, P = 0.5).
Conclusions: ADHF-CS is characterized by a higher prevalence of end-organ and biventricular dysfunction at presentation, a longer hospital length of stay, and higher need of heart replacement therapies when compared with AMI-CS. In-hospital mortality was similar between the two aetiologies. Our data warrant development of new management protocols focused on CS aetiology.
Keywords: Cardiogenic shock; Heart failure; Mortality; Myocardial infarction.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Nuccia Morici and Alice Sacco receives institutional grant support from Getinge Global US; Alice Sacco receives speaker honoraria from AstraZeneca and Menarini; Navin K. Kapur receives consulting/speaker honoraria and institutional grant support from Abbott Laboratories, Abiomed, Inc, Boston Scientific, Edwards, LivaNova, Getinge, Teleflex. and Zoll. Federico Pappalardo is a consultant for Abiomed. Fabrizio Oliva receives speaker honoraria from AstraZeneca, Viphor, Orion, and Novartis and has been involved in the advisory board of Novartis, AstraZeneca, and Bayer. Marco Marini receives consulting/speaker honoraria from AstraZeneca, Orion, and Abiomed. The other authors have nothing to declare.
Figures
References
-
- Chioncel O, Parissis J, Mebazaa A, Thiele H, Desch S, Bauersachs J, et al. Epidemiology, pathophysiology and contemporary management of cardiogenic shock—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2020;22:1315–1341. doi:10.1002/ejhf.1922 - DOI - PubMed
-
- Bertaina M, Galluzzo A, Rossello X, Sbarra P, Petitti E, Prever SB, et al. Prognostic implications of pulmonary artery catheter monitoring in patients with cardiogenic shock: A systematic review and meta‐analysis of observational studies. J Crit Care 2022;69:154024. doi:10.1016/j.jcrc.2022.154024 - DOI - PubMed
-
- Berg DD, Bohula EA, Van Diepen S, Katz JN, Alviar CL, Baird‐Zars VM, et al. Epidemiology of shock in contemporary cardiac intensive care units: Data from the critical care cardiology trials network registry. Circ Cardiovasc Qual Outcomes 2019;12:e005618. doi:10.1161/CIRCOUTCOMES.119.005618 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
