

Real-world costs of obesity-related complications over eight years: a US retrospective cohort study in 28,500 individuals
- PMID: 37723273
- PMCID: PMC10663144
- DOI: 10.1038/s41366-023-01376-4
Real-world costs of obesity-related complications over eight years: a US retrospective cohort study in 28,500 individuals
Abstract
Background: Obesity-related complications (ORCs) are associated with high costs for healthcare systems. We assessed the relationship between comorbidity burden, represented by both number and type of 14 specific ORCs, and total healthcare costs over time in people with obesity in the USA.
Methods: Adults (≥ 18 years old) identified from linked electronic medical records and administrative claims databases, with a body mass index measurement of 30-< 70 kg/m2 between 1 January 2007 and 31 March 2012 (earliest measurement: index date), and with continuous enrolment for ≥ 1 year pre index (baseline year) and ≥ 8 years post index, were included. Individuals were grouped by type and number of ORCs during the pre-index baseline year. The primary outcome was annual total adjusted direct per-person healthcare costs.
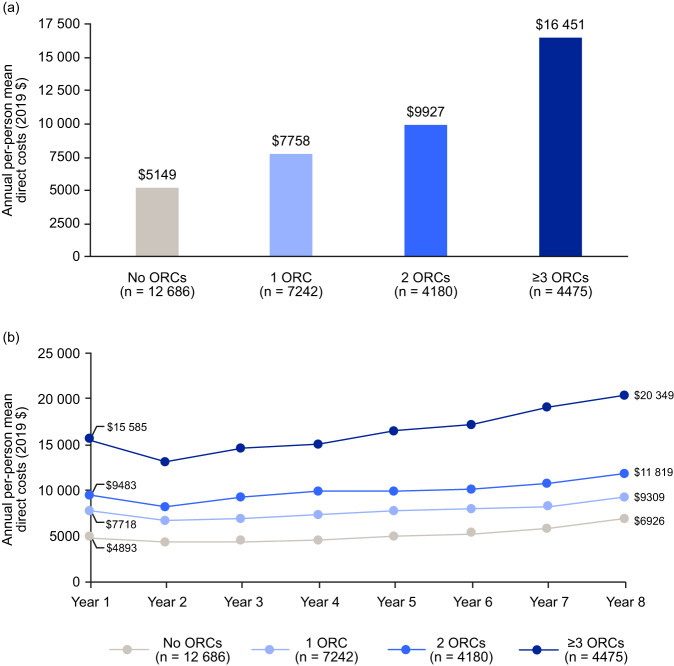
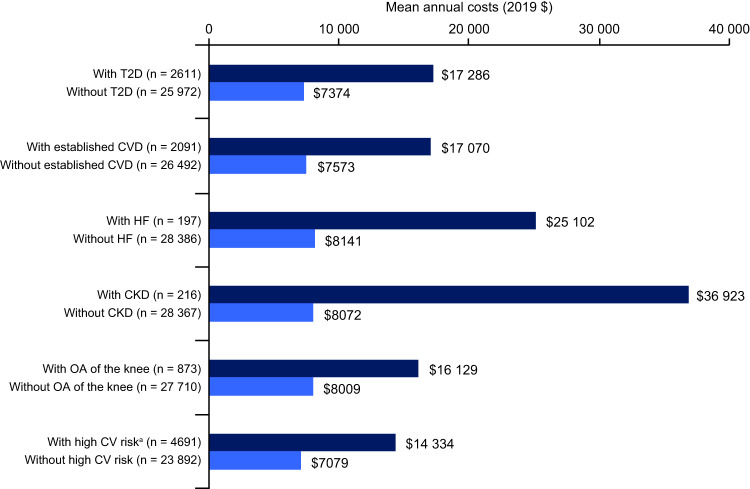
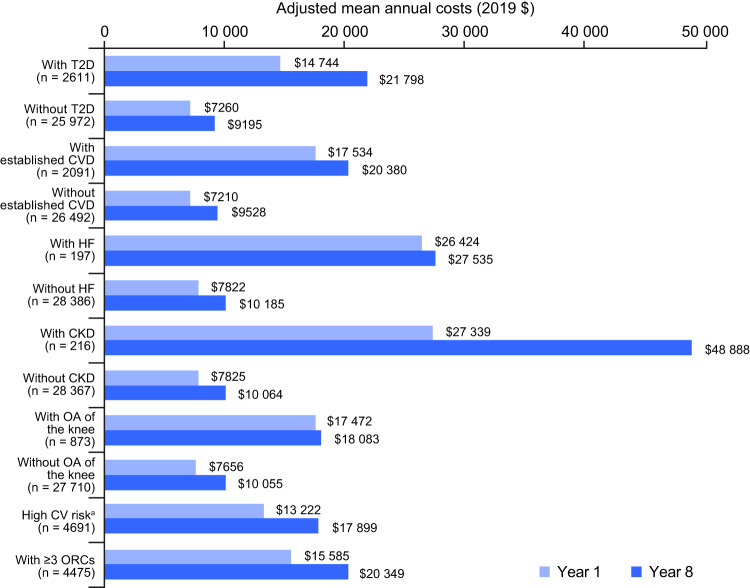
Results: Of 28,583 included individuals, 12,686 had no ORCs, 7242 had one ORC, 4180 had two ORCs and 4475 had three or more ORCs in the baseline year. Annual adjusted direct healthcare costs increased with the number of ORCs and over the 8-year follow-up. Outpatient costs were the greatest contributor to baseline annual direct costs, irrespective of the number of ORCs. For specific ORCs, costs generally increased gradually over the follow-up; the largest percentage increases from year 1 to year 8 were observed for chronic kidney disease (+ 78.8%) and type 2 diabetes (+ 47.8%).
Conclusions: In a US real-world setting, the number of ORCs appears to be a cost driver in people with obesity, from the time of initial obesity classification and for at least the following 8 years.
© 2023. The Author(s).
Conflict of interest statement
JP-S is partner and Head of Health Analytics at Lane Clark & Peacock LLP, Chair-elect of the Royal Society for Public Health and reports personal fees from Novo Nordisk A/S and Pfizer Ltd outside of the submitted work. SC, EdL, MF, CLH, and KSM are employees of Novo Nordisk A/S. AN, JT, and XZ are employees of IQVIA, and TB was an employee of IQVIA at the time the study was conducted; IQVIA received consulting fees from Novo Nordisk A/S to perform this analysis. ME has received fees from AstraZeneca, Boehringer Ingelheim and Novo Nordisk A/S.
Figures

Similar articles
-
Complication-specific direct medical costs by body mass index for 13 obesity-related complications: a retrospective database study.J Manag Care Spec Pharm. 2021 Feb;27(2):210-222. doi: 10.18553/jmcp.2020.20272. Epub 2020 Dec 14. J Manag Care Spec Pharm. 2021. PMID: 33307936 Free PMC article.
-
Eight-year trends in obesity-related complications and health care cost progression in a US population with obesity: A retrospective cohort study.Diabetes Obes Metab. 2023 Feb;25(2):536-544. doi: 10.1111/dom.14897. Epub 2022 Nov 7. Diabetes Obes Metab. 2023. PMID: 36263756
-
Prevalence and healthcare costs of obesity-related comorbidities: evidence from an electronic medical records system in the United States.J Med Econ. 2015;18(12):1020-8. doi: 10.3111/13696998.2015.1067623. Epub 2015 Sep 4. J Med Econ. 2015. PMID: 26134917
-
Ten-year progression of obesity-related complications in a population with overweight and obesity in the UK: A retrospective open cohort study.Diabetes Obes Metab. 2024 Nov;26(11):5056-5064. doi: 10.1111/dom.15836. Epub 2024 Aug 19. Diabetes Obes Metab. 2024. PMID: 39159940
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
Cited by
-
Effectiveness of a Food Education Program for healthcare workers: a pilot study in a Total Worker Health© approach.Front Public Health. 2025 Mar 12;13:1523131. doi: 10.3389/fpubh.2025.1523131. eCollection 2025. Front Public Health. 2025. PMID: 40144992 Free PMC article.
-
Prevalence of obesity-related multimorbidity and its health care costs among adults in the United States.J Manag Care Spec Pharm. 2025 Feb 1;31(2):179-188. doi: 10.18553/jmcp.2025.31.2.179. J Manag Care Spec Pharm. 2025. PMID: 39912809 Free PMC article.
-
Association between adolescent obesity and early adulthood healthcare utilization-a two-cohort prospective study.BMC Med. 2025 Jan 21;23(1):33. doi: 10.1186/s12916-025-03866-w. BMC Med. 2025. PMID: 39838331 Free PMC article.
-
Management and impact of obesity in Canada: A real-world survey of people with obesity and their physicians.Obes Pillars. 2025 Feb 28;14:100171. doi: 10.1016/j.obpill.2025.100171. eCollection 2025 Jun. Obes Pillars. 2025. PMID: 40134800 Free PMC article.
-
Liver steatosis is positively associated with plasminogen activator inhibitor-1 in apparently healthy individuals with overweight and obesity: A FibroScan-Based Cross-Sectional study.J Transl Med. 2025 Apr 29;23(1):487. doi: 10.1186/s12967-025-06464-9. J Transl Med. 2025. PMID: 40301952 Free PMC article.
References
-
- World Health Organization. Obesity and overweight. 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 1 June 2022.
-
- Centers for Disease Control and Prevention. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. 2020. https://www.cdc.gov/nchs/products/databriefs/db360.htm. Accessed 6 January 2022.
-
- Lange SJ, Kompaniyets L, Freedman DS, Kraus EM, Porter R, Blanck HM, et al. Longitudinal trends in body mass index before and during the COVID-19 pandemic among persons aged 2–19 years — United States, 2018–2020. MMWR Morb Mortal Wkly Rep. 2021;70:1278–83.. doi: 10.15585/mmwr.mm7037a3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
