

Angiography-based hemodynamic features predict recurrent ischemic events after angioplasty and stenting of intracranial vertebrobasilar atherosclerotic stenosis
- PMID: 37723287
- PMCID: PMC10957605
- DOI: 10.1007/s00330-023-10209-x
Angiography-based hemodynamic features predict recurrent ischemic events after angioplasty and stenting of intracranial vertebrobasilar atherosclerotic stenosis
Abstract
Objectives: To assess the predictive value of hemodynamic features for stroke relapse in patients with intracranial vertebrobasilar atherosclerotic stenosis treated with percutaneous transluminal angioplasty and stenting (PTAS) using quantitative digital subtraction angiography (q-DSA).
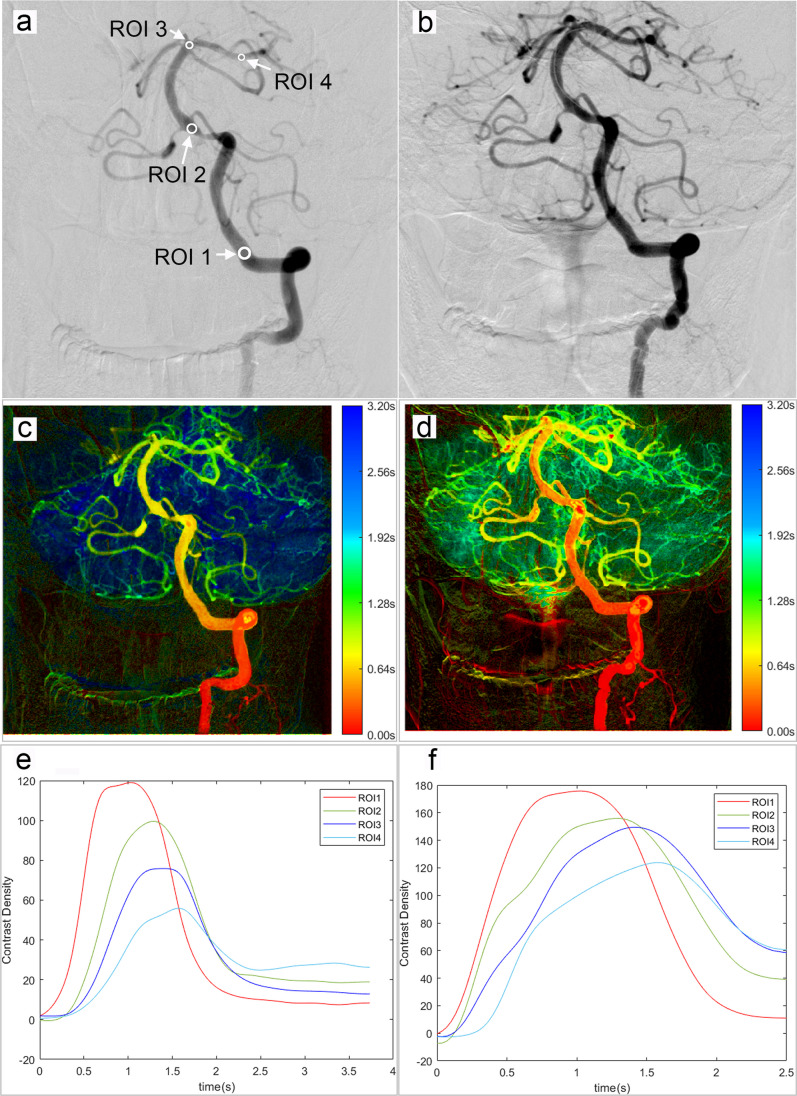
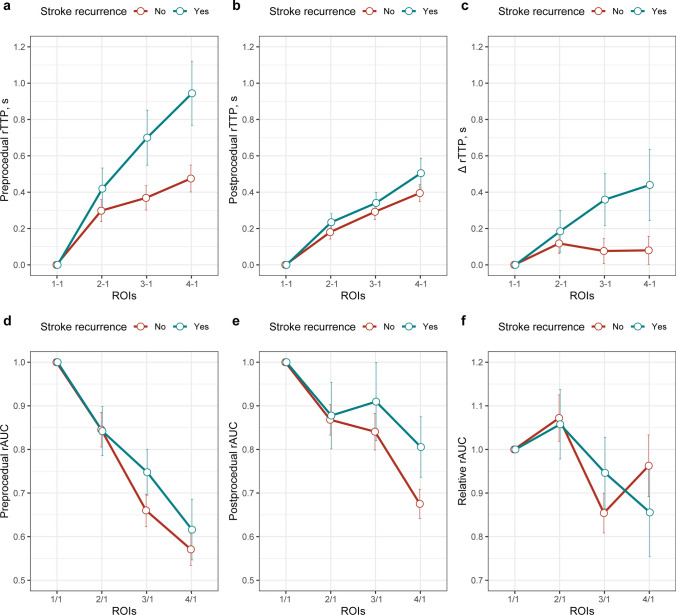
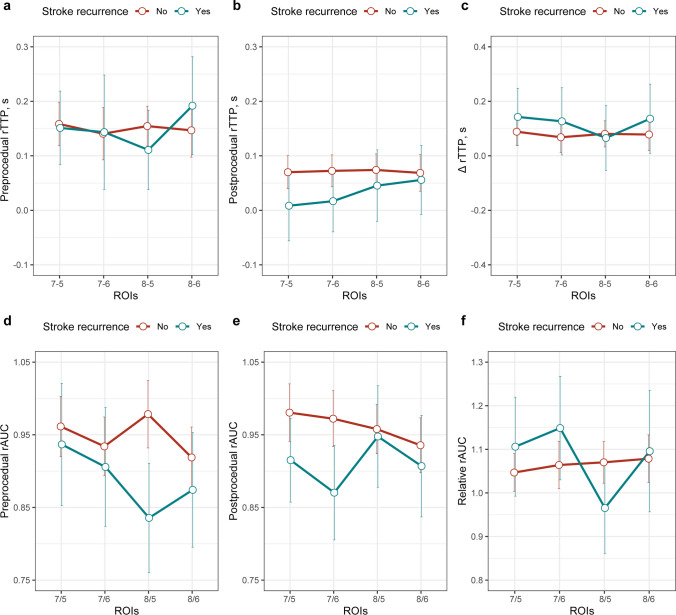
Methods: In this retrospective longitudinal study, patients with intracranial vertebrobasilar atherosclerotic stenosis and who underwent PTAS treatment between January 2012 and May 2020 were enrolled. The q-DSA assessment was performed before and after PTAS. ROIs 1-4 were placed along the vertebral artery, proximal and distal basilar artery, and posterior cerebral artery; ROIs 5-8 were in 5 mm and 10 mm proximal and distal to the lesion, respectively. Relative time to peak (rTTP) was defined as the difference in TTP between ROIs. Cox regression analyses were performed to determine risk factors for recurrent stroke.
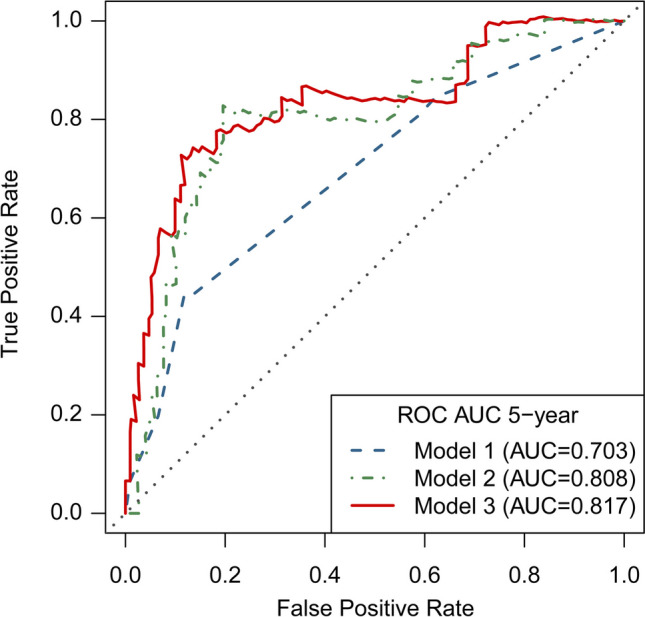
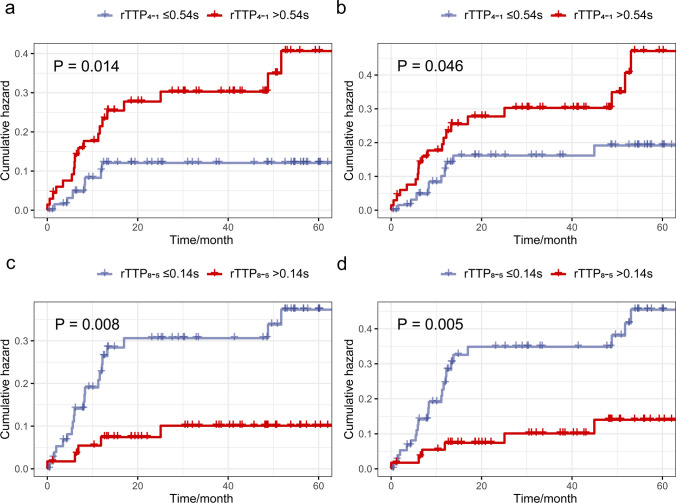
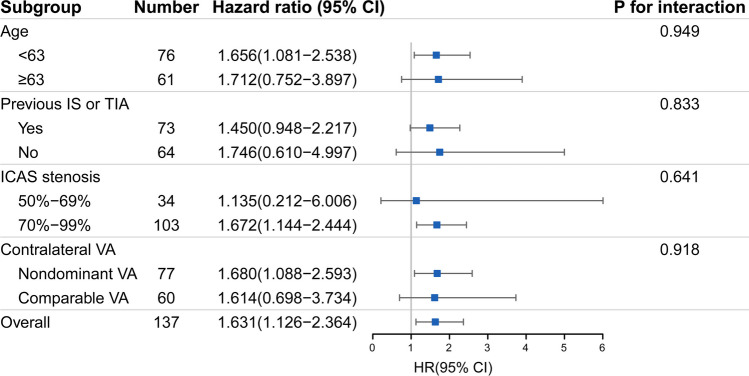
Results: A total of 137 patients (mean age, 62 years ± 10 [standard deviation], 83.2% males) were included, and 26 (19.0%) patients had stroke relapse during follow-up (median time of 42.6 months [interquartile range, 19.7-60.7]). Preprocedural rTTP4-1 (adjusted hazard ratio (HR) = 2.270; 95% CI 1.371-3.758; p = 0.001) and preprocedural rTTP8-5 (adjusted HR = 0.240; 95% CI 0.088-0.658; p = 0.006) were independently associated with the recurrent stroke. These hemodynamic parameters provided an incremental prognostic value for stroke relapse (AUC, 0.817 [0.704-0.931]; the net reclassification index, 0.431 [0.057-0.625]; and the integrated discrimination index, 0.140 [0.035-0.292]).
Conclusions: In patients with intracranial vertebrobasilar atherosclerosis treated with PTAS, preprocedural prolonged TTP of the target vessel and shortened trans-stenotic TTP difference were associated with stroke relapse. Q-DSA-defined hemodynamic parameters provided incremental predictive value over conventional parameters for stroke recurrence.
Clinical relevance statement: Quantitative DSA analysis enables intuitive observation and semi-quantitative evaluation of peri-therapeutic cerebral blood flow. More importantly, quantitative DSA-defined hemodynamic parameters have the potential for risk stratification of patients with intracranial atherosclerotic stenosis.
Key points: Semi-quantitative angiography-based parameters can reflect pre- and postprocedural subtle changes in blood flow in patients with intracranial atherosclerotic stenosis. Although angioplasty procedures can significantly improve blood flow status, patients with more restricted baseline blood flow still show a higher risk of stroke recurrence. Angiography-based hemodynamic features possess prognostic value and can serve as clinical markers to assess stroke risk of patients with intracranial atherosclerotic stenosis.
Keywords: Cerebral angiography; Hemodynamics; Intracranial atherosclerosis; Recurrence; Stroke.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
Yan Xu is an employee of Neusoft Medical Systems Co., Ltd., Shenyang, China. Dr. Zhongzhao Teng is the chief scientist of Tenoke Ltd., Cambridge, UK, and Nanjing Jingsan Medical Science and Technology, Ltd., Nanjing, China.
Other authors do not have any conflict of interest to disclose.
Figures
Similar articles
-
Percutaneous transluminal angioplasty and stenting (PTAS) in patients with symptomatic intracranial vertebrobasilar artery stenosis (IVBS).Stroke Vasc Neurol. 2025 Apr 29;10(2):e003224. doi: 10.1136/svn-2024-003224. Stroke Vasc Neurol. 2025. PMID: 39168503 Free PMC article.
-
Natural History of Hemodynamics in Vertebrobasilar Disease: Temporal Changes in the VERiTAS Study Cohort.Stroke. 2020 Nov;51(11):3295-3301. doi: 10.1161/STROKEAHA.120.029909. Epub 2020 Oct 9. Stroke. 2020. PMID: 33032489 Free PMC article.
-
Hemodynamic alterations in unilateral chronic middle cerebral artery stenosis patients and the effect of percutaneous transluminal angioplasty and stenting: a perfusion-computed tomography study.Acta Radiol. 2015 Jun;56(6):754-60. doi: 10.1177/0284185114538793. Epub 2014 Jul 9. Acta Radiol. 2015. PMID: 25009278
-
Symptomatic intracranial vertebral artery atherosclerotic stenosis (≥70%) with concurrent contralateral vertebral atherosclerotic diseases in 88 patients treated with the intracranial stenting.Eur J Radiol. 2015 Sep;84(9):1801-4. doi: 10.1016/j.ejrad.2015.05.033. Epub 2015 Jun 5. Eur J Radiol. 2015. PMID: 26119803
-
Long-Term Evolutionary Change in the Lumen of Intracranial Atherosclerotic Stenosis Following Angioplasty and Stenting.Oper Neurosurg. 2018 Feb 1;14(2):128-138. doi: 10.1093/ons/opx097. Oper Neurosurg. 2018. PMID: 28637237 Review.
Cited by
-
Can high-resolution magnetic resonance-vessel wall imaging simplify moyamoya disease assessment?Eur Radiol. 2023 Oct;33(10):6916-6917. doi: 10.1007/s00330-023-10088-2. Epub 2023 Aug 10. Eur Radiol. 2023. PMID: 37561184 No abstract available.
-
Endovascular Treatment of Symptomatic Basilar Artery Stenosis.Neurointervention. 2023 Nov;18(3):166-171. doi: 10.5469/neuroint.2023.00437. Epub 2023 Oct 19. Neurointervention. 2023. PMID: 37853573 Free PMC article.
-
Spinal cord infarction after stenting for symptomatic severe stenosis of the basilar artery: a case description and literature analysis.Quant Imaging Med Surg. 2025 Aug 1;15(8):7634-7644. doi: 10.21037/qims-2025-332. Epub 2025 Jul 29. Quant Imaging Med Surg. 2025. PMID: 40785914 Free PMC article. No abstract available.
-
Higher Time to Peak after Stent Implantation in Symptomatic High-Grade Intracranial Atherosclerotic Stenosis is Related to In-Stent Restenosis.Transl Stroke Res. 2025 Mar 22. doi: 10.1007/s12975-025-01346-0. Online ahead of print. Transl Stroke Res. 2025. PMID: 40120037
-
Integrating hemodynamic analysis with traditional imaging in intracranial atherosclerotic stenosis: current status and future perspectives.Front Neurol. 2025 Jul 18;16:1589162. doi: 10.3389/fneur.2025.1589162. eCollection 2025. Front Neurol. 2025. PMID: 40757026 Free PMC article. Review.
References
MeSH terms
Grants and funding
- U20A20357/the National natural science foundation of China
- 81870946/the National natural science foundation of China
- WK9110000056/Fundamental Research Funds for Central Universities of the Central South University
- BE2020700/Jiangsu Provincial Key Research and Development Program
- BE2020697/Jiangsu Provincial Key Research and Development Program
LinkOut - more resources
Full Text Sources
Medical
