Management and rehabilitation of moderate-to-severe diabetic foot infection: a narrative review
- PMID: 37723835
- PMCID: PMC10626302
- DOI: 10.12701/jyms.2023.00717
Management and rehabilitation of moderate-to-severe diabetic foot infection: a narrative review
Abstract
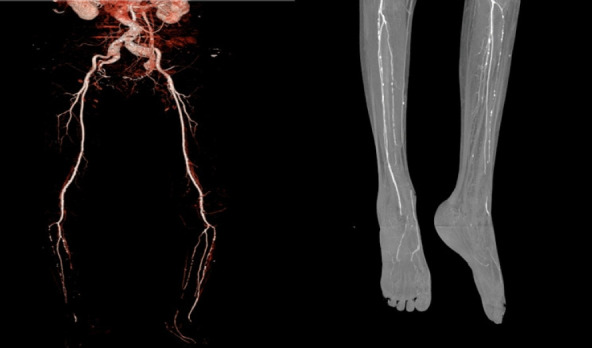
Diabetic foot is one of the most devastating consequences of diabetes, resulting in amputation and possibly death. Therefore, early detection and vigorous treatment of infections in patients with diabetic foot are critical. This review seeks to provide guidelines for the therapy and rehabilitation of patients with moderate-to-severe diabetic foot. If a diabetic foot infection is suspected, bacterial cultures should be initially obtained. Numerous imaging studies can be used to identify diabetic foot, and recent research has shown that white blood cell single-photon emission computed tomography/computed tomography has comparable diagnostic specificity and sensitivity to magnetic resonance imaging. Surgery is performed when a diabetic foot ulcer is deep and is accompanied by bone and soft tissue infections. Patients should be taught preoperative rehabilitation before undergoing stressful surgery. During surgical procedures, it is critical to remove all necrotic tissue and drain the inflammatory area. It is critical to treat wounds with suitable dressings after surgery. Wet dressings promote the formation of granulation tissues and new blood vessels. Walking should begin as soon as the patient's general condition allows it, regardless of the wound status or prior walking capacity. Adequate treatment of comorbidities, including hypertension and dyslipidemia, and smoking cessation are necessary. Additionally, broad-spectrum antibiotics are required to treat diabetic foot infections.
Keywords: Diabetes mellitus; Diabetic foot; Management; Rehabilitation.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures



Similar articles
-
Diagnosis and treatment of diabetic foot infections.Plast Reconstr Surg. 2006 Jun;117(7 Suppl):212S-238S. doi: 10.1097/01.prs.0000222737.09322.77. Plast Reconstr Surg. 2006. PMID: 16799390
-
Poorly designed research does not help clarify the role of hyperbaric oxygen in the treatment of chronic diabetic foot ulcers.Diving Hyperb Med. 2016 Sep;46(3):133-134. Diving Hyperb Med. 2016. PMID: 27723012
-
Effect of leukocyte-platelet fibrin-rich wound reconstruction followed by full-thickness skin grafting in the treatment of diabetic foot Wagner grade 4 ulcer gangrene (toe area).Platelets. 2023 Dec;34(1):2131752. doi: 10.1080/09537104.2022.2131752. Epub 2022 Oct 10. Platelets. 2023. PMID: 36210791
-
[Multidisciplinary management of diabetic foot ulcer infection].Rev Med Interne. 2021 Mar;42(3):193-201. doi: 10.1016/j.revmed.2020.09.004. Epub 2021 Jan 12. Rev Med Interne. 2021. PMID: 33451819 Review. French.
-
Autolytic debridement of a large, necrotic, fully occluded foot ulcer using a hydrocolloid dressing in a diabetic patient.Adv Skin Wound Care. 2013 Jul;26(7):300-4. doi: 10.1097/01.ASW.0000429779.48138.c0. Adv Skin Wound Care. 2013. PMID: 23777879 Review.
Cited by
-
Unveiling the challenges of diabetic foot infections: diagnosis, pathogenesis, treatment, and rehabilitation.J Yeungnam Med Sci. 2023 Oct;40(4):319-320. doi: 10.12701/jyms.2023.01011. Epub 2023 Oct 11. J Yeungnam Med Sci. 2023. PMID: 37817464 Free PMC article. No abstract available.
References
-
- Lee CW. Diagnosis and management of diabetic foot. J Korean Diabetes. 2018;19:168–74.
-
- Bae SY. Treatment of diabetic foot: procedures, surgery, and care. Monthly Diabetes. 2013;289:26–36.
-
- Armstrong DG, Wrobel J, Robbins JM. Guest Editorial: are diabetes-related wounds and amputations worse than cancer? Int Wound J. 2007;4:286–7. - PubMed
-
- Ahn KJ. Epidemiology of diabetic foot disease. J Korean Diabetes. 2011;12:72–5.
Grants and funding
LinkOut - more resources
Full Text Sources