

Acquired risk factors and incident atrial fibrillation according to age and genetic predisposition
- PMID: 37723974
- PMCID: PMC10719493
- DOI: 10.1093/eurheartj/ehad615
Acquired risk factors and incident atrial fibrillation according to age and genetic predisposition
Abstract
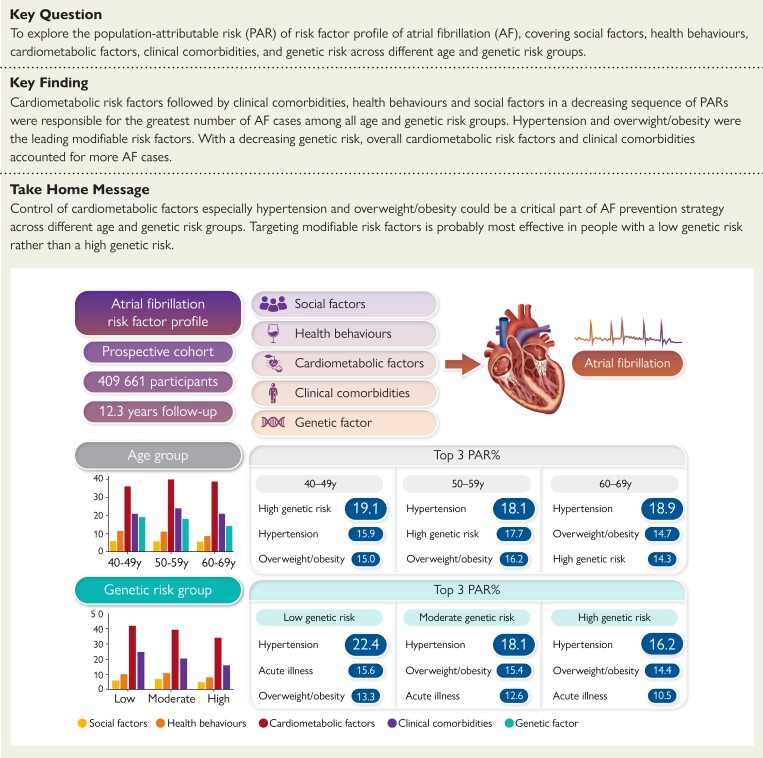
Background and aims: Atrial fibrillation (AF) is the most common sustained arrhythmia in adults. Investigations of risk factor profiles for AF according to age and genetic risk groups are essential to promote individualized strategies for the prevention and control of AF.
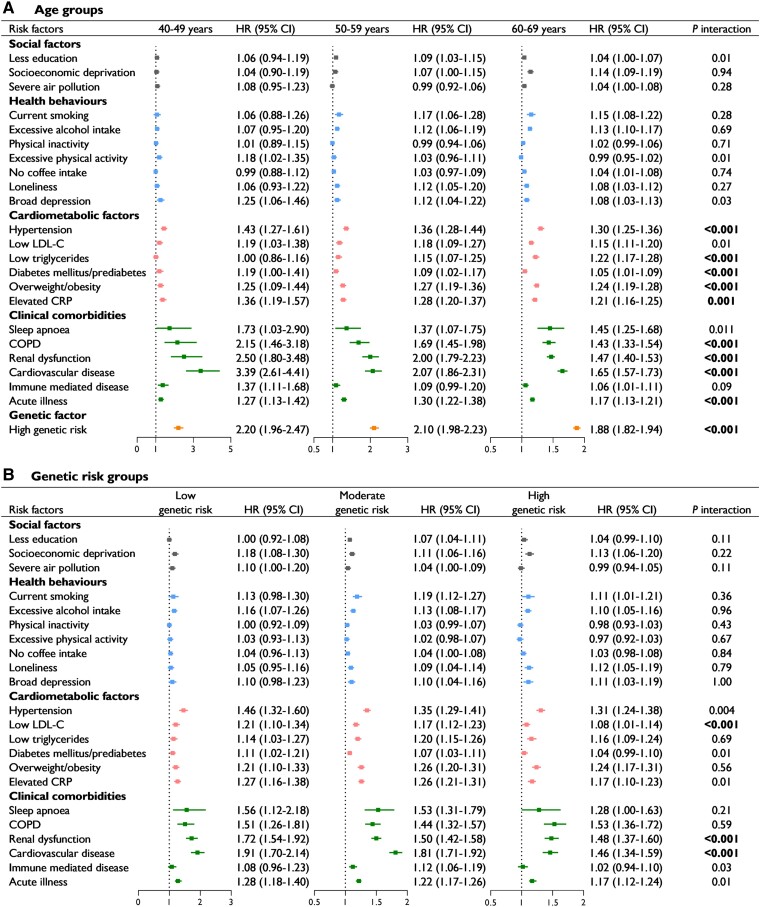
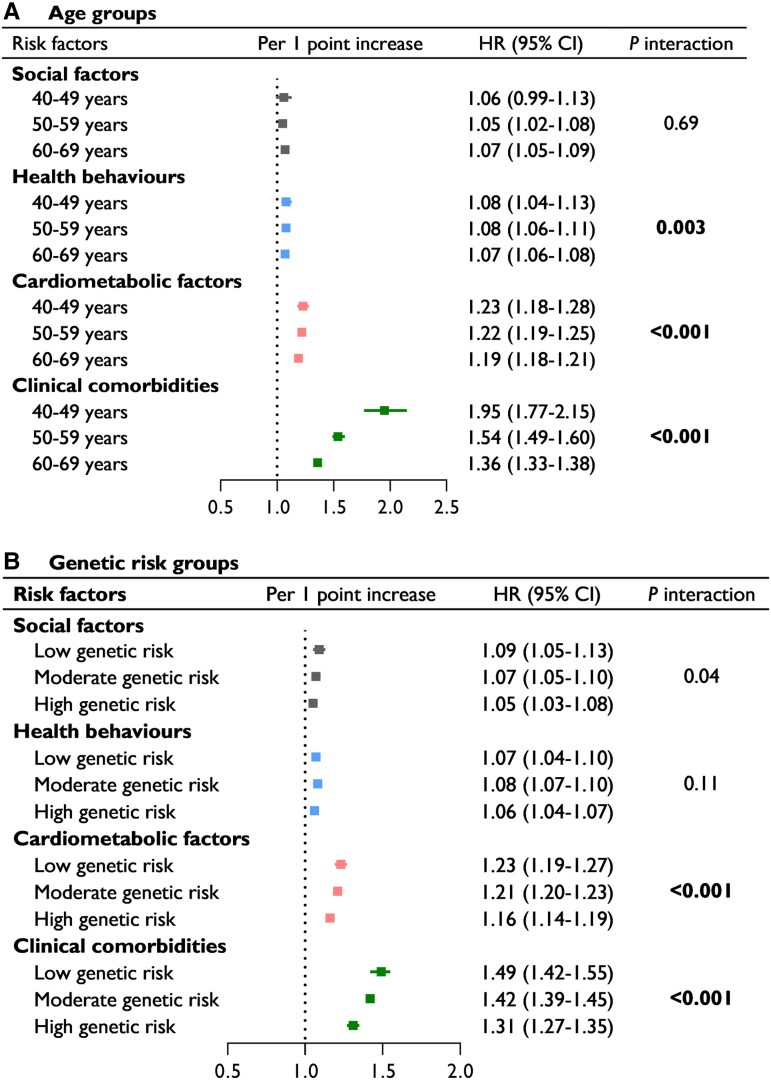
Methods: A total of 409 661 participants (mean age, 56 years; 46% men) free of AF at baseline and with complete information about risk factors were included from the UK Biobank cohort. The hazard ratios and population-attributable risk (PAR) percentages of incident AF associated with 23 risk factors were examined, including 3 social factors, 7 health behaviours, 6 cardiometabolic factors, 6 clinical comorbidities, and the genetic risk score (GRS), across 3 age groups (40-49, 50-59, and 60-69 years) and 3 genetic risk groups (low, moderate, and high GRS).
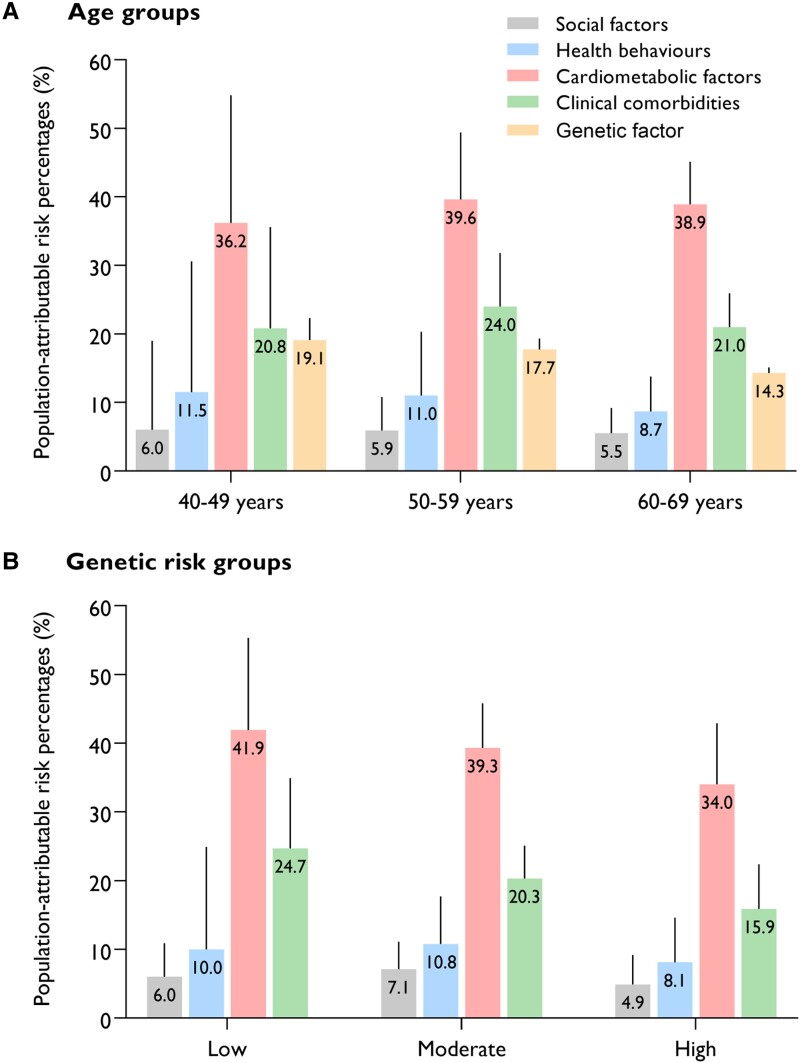
Results: After a follow-up of 5 027 587 person-years, 23 847 participants developed AF. Most cardiometabolic factors and clinical comorbidities showed a significant interaction with age, whereby the associations were generally strengthened in younger groups (Pinteraction < .002). However, only low LDL cholesterol, renal dysfunction, and cardiovascular disease showed a significant interaction with genetic risk, and the associations with these factors were stronger in lower genetic risk groups (Pinteraction < .002). Cardiometabolic factors consistently accounted for the largest number of incident AF cases across all age groups (PAR: 36.2%-38.9%) and genetic risk groups (34.0%-41.9%), with hypertension and overweight/obesity being the two leading modifiable factors. Health behaviours (PAR: 11.5% vs. 8.7%) and genetic risk factors (19.1% vs. 14.3%) contributed to more AF cases in the 40-49 years group than in the 60-69 years group, while the contribution of clinical comorbidities remained relatively stable across different age groups. The AF risk attributable to overall cardiometabolic factors (PAR: 41.9% in the low genetic risk group and 34.0% in the high genetic risk group) and clinical comorbidities (24.7% and 15.9%) decreased with increasing genetic risk. The impact of social factors on AF was relatively low across the groups by age and genetic risk.
Conclusions: This study provided comprehensive information about age- and genetic predisposition-related risk factor profiles for AF in a cohort of UK adults. Prioritizing risk factors according to age and genetic risk stratifications may help to achieve precise and efficient prevention of AF.
Keywords: Age; Atrial fibrillation; Genetic risk; Risk profile; UK Biobank.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Comment in
-
Prevention of atrial fibrillation: a call to action.Eur Heart J. 2023 Dec 14;44(47):4994-4996. doi: 10.1093/eurheartj/ehad738. Eur Heart J. 2023. PMID: 37919240 Free PMC article. No abstract available.
Comment on
-
Prevention of atrial fibrillation: a call to action.Eur Heart J. 2023 Dec 14;44(47):4994-4996. doi: 10.1093/eurheartj/ehad738. Eur Heart J. 2023. PMID: 37919240 Free PMC article. No abstract available.
References
-
- Staerk L, Wang B, Preis SR, Larson MG, Lubitz SA, Ellinor PT, et al. Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: cohort study based on longitudinal data from the Framingham Heart Study. BMJ 2018;361:k1453. 10.1136/bmj.k1453 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
