

Histological findings associated with treatment response in cutaneous leishmaniasis: a clinicopathological correlation study
- PMID: 37723978
- PMCID: PMC10516507
- DOI: 10.1111/ijd.16826
Histological findings associated with treatment response in cutaneous leishmaniasis: a clinicopathological correlation study
Abstract
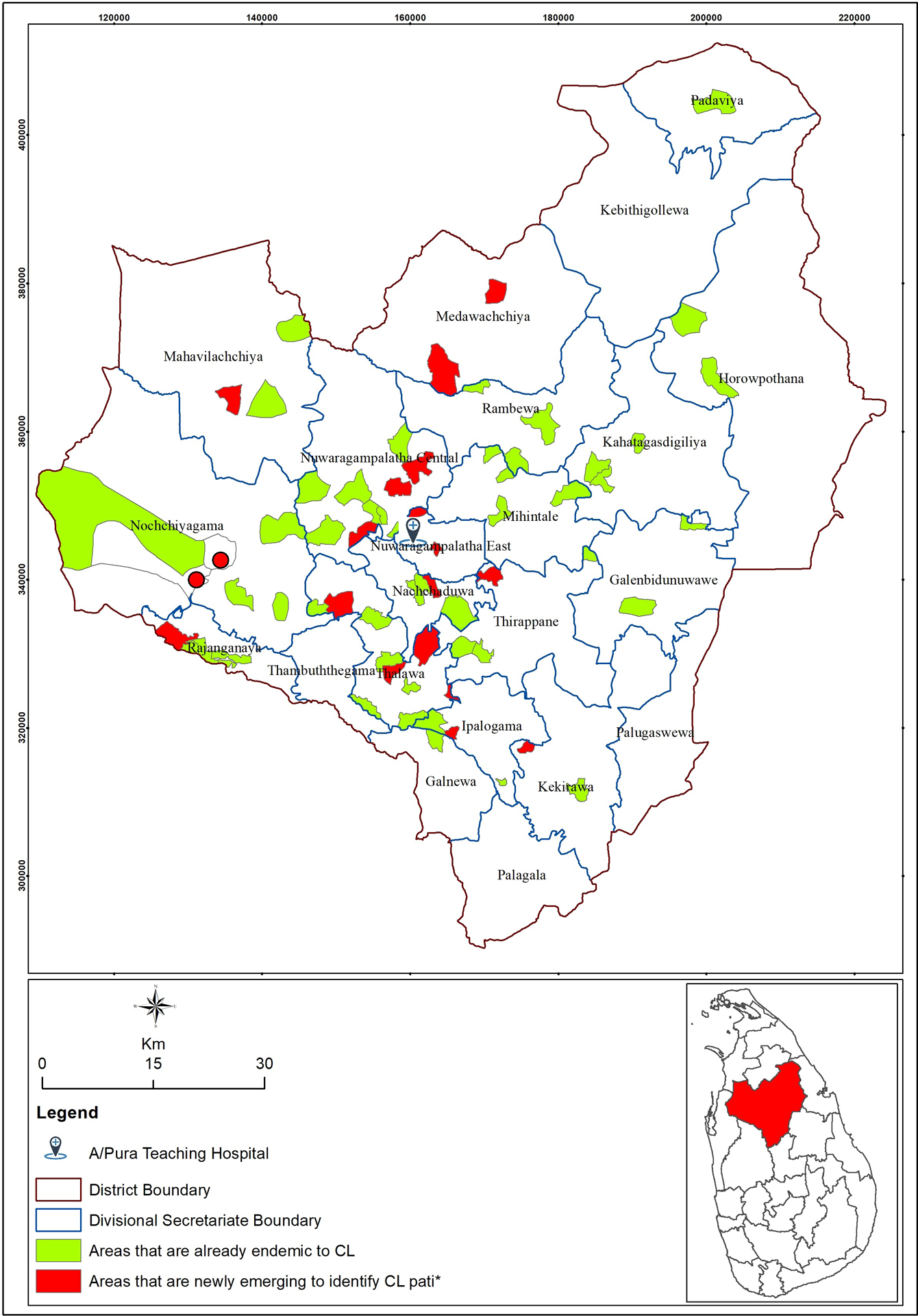
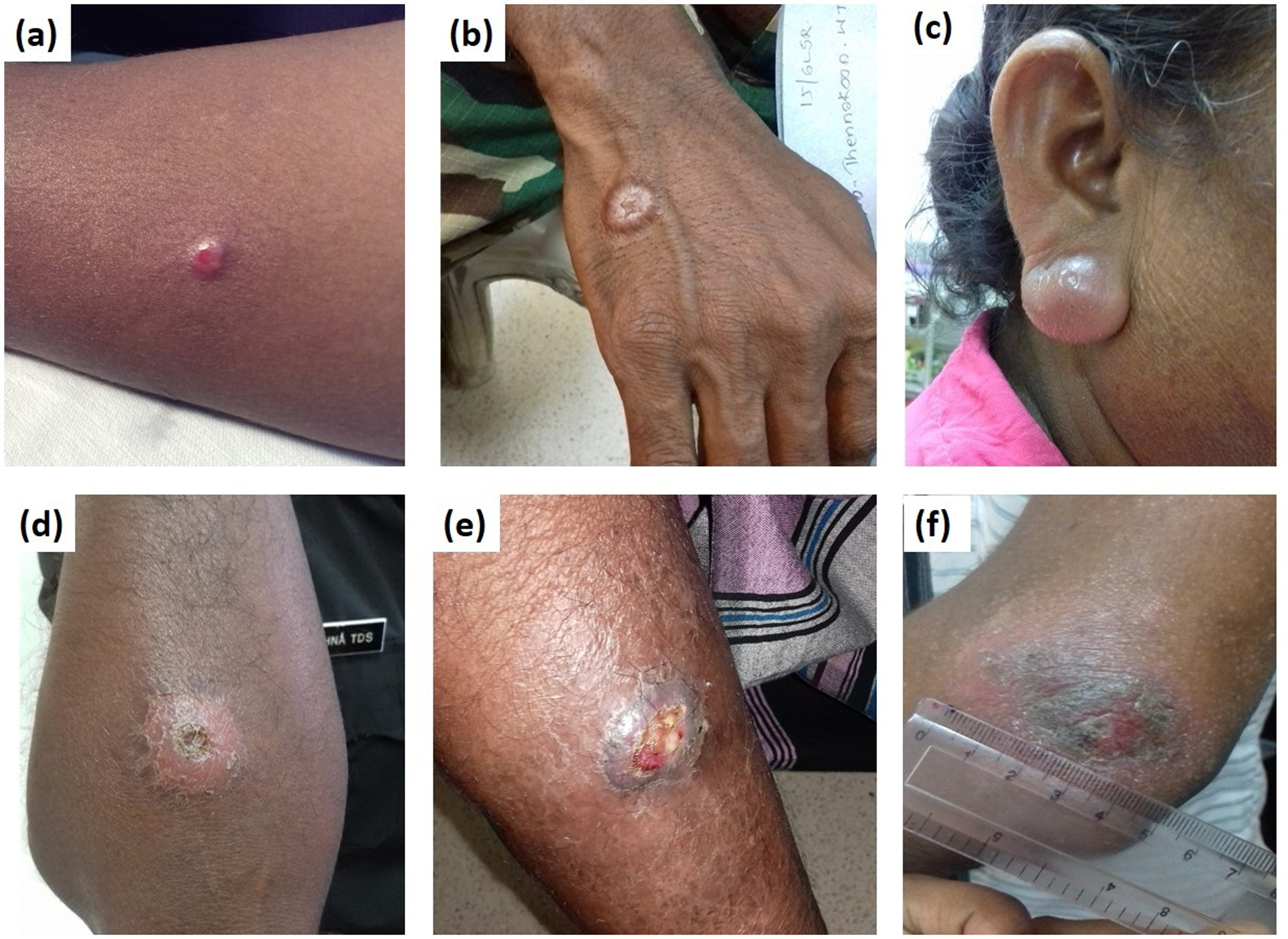
Background: Treatment responses to cutaneous leishmaniasis (CL) observed in Sri Lanka show variability, ranging from quick healing to delayed or failed responses to routine medication. The determinants of these differences in treatment response are not well defined. This study aimed to identify predictive features of treatment response and outcome in localized CL caused by Leishmania donovani, focusing on both clinical and histopathological findings in the patients.
Methods: Tissue sections (n = 103) derived from 3 mm punch biopsies of parasitologically confirmed patients were assessed. Patients were followed up weekly until complete healing of skin lesions and were reviewed at the end of 6 months and 1 year.
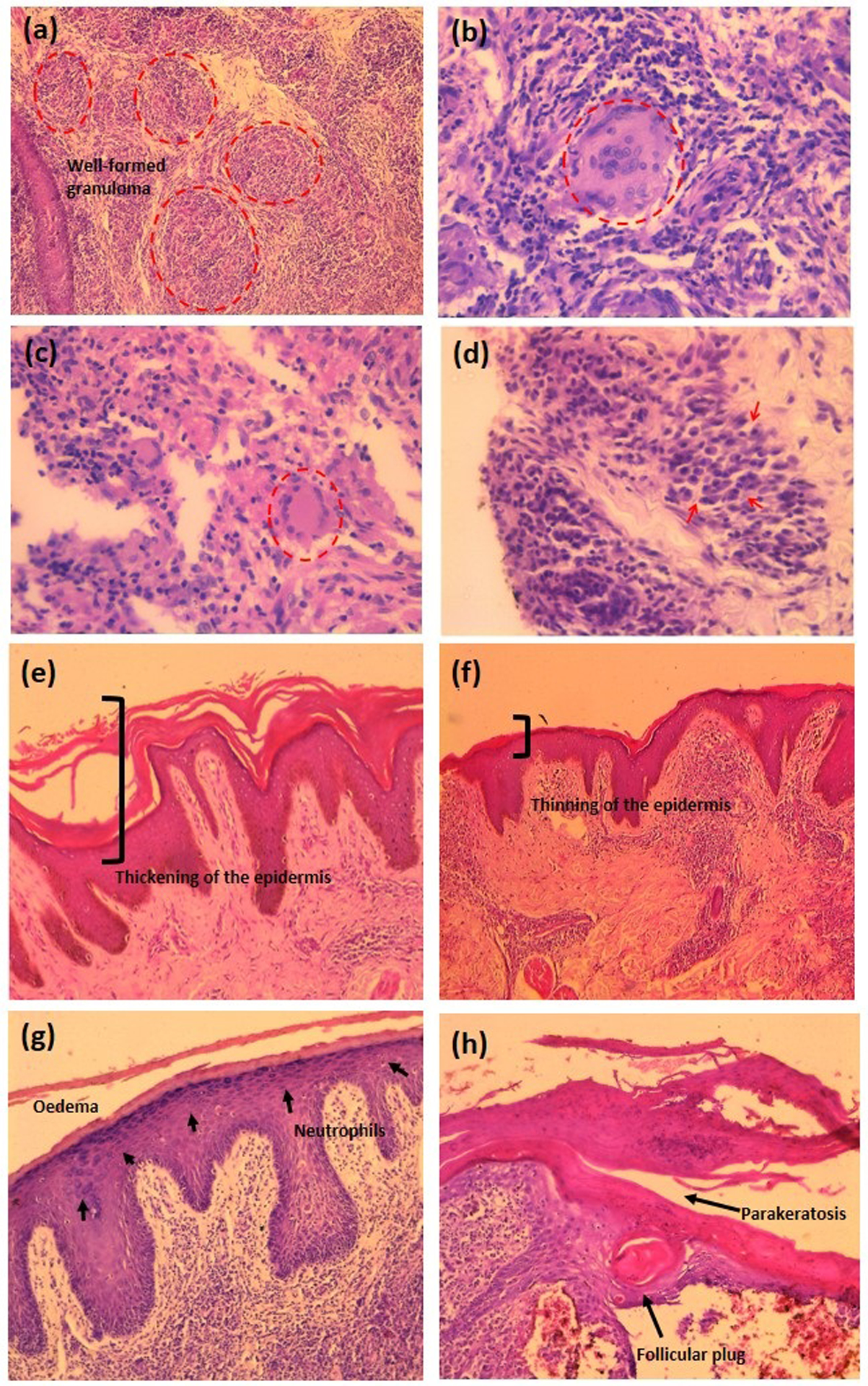
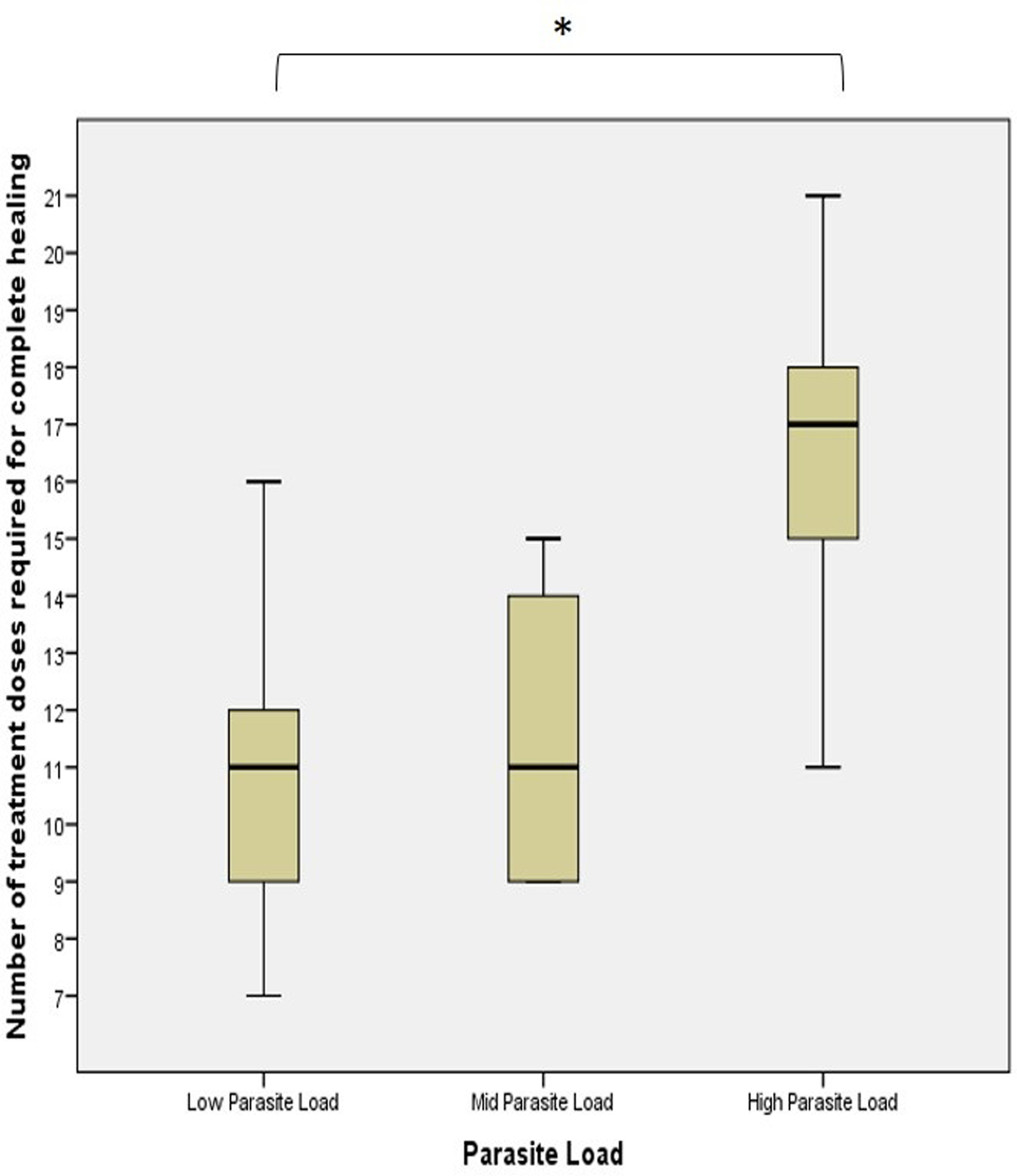
Results: Healing required 7-21 weekly doses of intralesional sodium stibogluconate (IL-SSG) (mean = 12.2 ± 0.622). Twenty-nine (28.1%) patients were identified as delayed responders. None had recurred at the end of 1 year. The demographic or clinical features (age, gender, lesion type, size, location, and lesion duration) did not significantly influence the treatment response. A heavy parasite load and acanthosis were significant predictors of a delayed response to treatment (P < 0.001). Higher parasite loads were associated with inflammation of the entire dermis (P = 0.008), more intense infiltration of macrophages (p = 0.001), and epidermal atrophy (P = 0.033). Well-formed granulomas were inversely proportional to parasite loads.
Conclusions: Histology findings proved to be better prognostic markers than clinical features for delayed responders to treatment and will aid in targeted patient management when tissue biopsies are performed in the initial diagnosis of CL.
© 2023 the International Society of Dermatology.
Conflict of interest statement
Figures

References
-
- Desjeux P Leishmaniasis: Current situation and new perspectives. Comp Immunol Microbiol Infect Dis 2004;27:305–18. - PubMed
-
- Athukorale DN, Seneviratne JK, Ihalamulla RL PU. Locally acquired cutaneous leishmaniasis in Sri Lanka. J Trop Med Hyg 1992;95:432–3. - PubMed
-
- Karunaweera ND, Pratlong F, Siriwardane HVYD, Ihalamulla RL, Dedet JP. Sri Lankan cutaneous leishmaniasis is caused by Leishmania donovani zymodeme MON-37. Trans R Soc Trop Med Hyg 2003;97:380–1. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
