

Post-traumatic stress disorder: a psychiatric disorder requiring urgent attention
- PMID: 37724188
- PMCID: PMC10388753
- DOI: 10.1515/mr-2022-0012
Post-traumatic stress disorder: a psychiatric disorder requiring urgent attention
Abstract
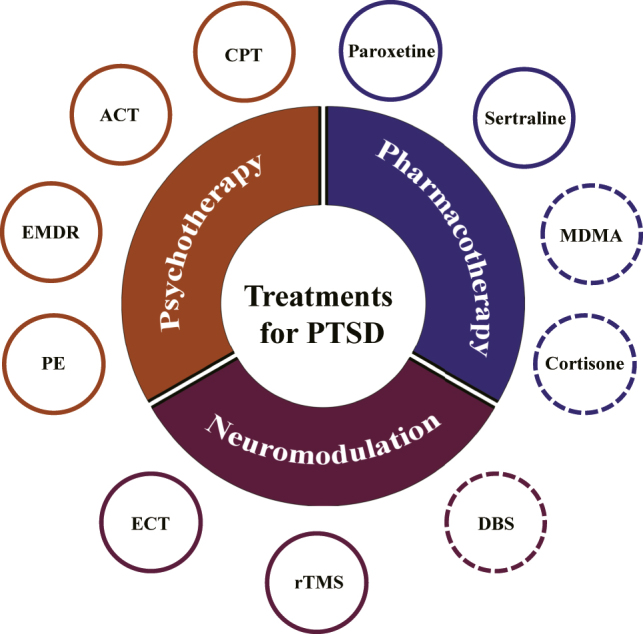
Post-traumatic stress disorder (PTSD) is a severe and heterogenous psychiatric disorder that was first defined as a mental disorder in 1980. Currently, the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) and the International Classification of Diseases 11th Edition (ICD-11) offer the most widely accepted diagnostic guidelines for PTSD. In both diagnostic categories, experiencing a traumatic event (TE) is the necessary criterion for diagnosing PTSD. The TEs described in the DSM-5 include actual or threatened death, serious injury, sexual violence, and other extreme stressors, either directly or indirectly. More than 70% of adults worldwide are exposed to a TE at least once in their lifetime, and approximately 10% of individuals develop PTSD after experiencing a TE. The important features of PTSD are intrusion or re-experiencing fear memories, pervasive sense of threat, active avoidance, hyperarousal symptoms, and negative alterations of cognition and mood. Individuals with PTSD have high comorbidities with other psychiatric diseases, including major depressive disorder, generalized anxiety disorder, and substance use disorder. Multiple lines of evidence suggest that the pathophysiology of PTSD is complex, involving abnormal neural circuits, molecular mechanisms, and genetic mechanisms. A combination of both psychotherapy and pharmacotherapy is used to treat PTSD, but has limited efficacy in patients with refractory PTSD. Because of the high prevalence, heavy burden, and limited treatments, PTSD is a psychiatric disorder that requires urgent attention. In this review, we summarize and discuss the diagnosis, prevalence, TEs, pathophysiology, and treatments of PTSD and draw attention to its prevention.
Keywords: animal models; comorbidity; pathophysiology; post-traumatic stress disorder; traumatic events; treatments.
© 2022 the author(s), published by De Gruyter, Berlin/Boston.
Conflict of interest statement
Competing interests: Authors have no conflict of interest to declare.
Figures






Similar articles
-
Letter to the Editor: CONVERGENCES AND DIVERGENCES IN THE ICD-11 VS. DSM-5 CLASSIFICATION OF MOOD DISORDERS.Turk Psikiyatri Derg. 2021;32(4):293-295. doi: 10.5080/u26899. Turk Psikiyatri Derg. 2021. PMID: 34964106 English, Turkish.
-
Nabilone for the Treatment of Post-Traumatic Stress Disorder: A Review of Clinical Effectiveness and Guidelines [Internet].Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2019 Feb 20. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2019 Feb 20. PMID: 31553551 Free Books & Documents. Review.
-
Comorbidity of developmental trauma disorder (DTD) and post-traumatic stress disorder: findings from the DTD field trial.Eur J Psychotraumatol. 2019 Jan 29;10(1):1562841. doi: 10.1080/20008198.2018.1562841. eCollection 2019. Eur J Psychotraumatol. 2019. PMID: 30728917 Free PMC article.
-
[Post-traumatic stress, post-traumatic depression and major depressive episode: literature].Encephale. 2001 Mar-Apr;27(2):159-68. Encephale. 2001. PMID: 11407268 Review. French.
-
Human brain evolution and the "Neuroevolutionary Time-depth Principle:" Implications for the Reclassification of fear-circuitry-related traits in DSM-V and for studying resilience to warzone-related posttraumatic stress disorder.Prog Neuropsychopharmacol Biol Psychiatry. 2006 Jul;30(5):827-53. doi: 10.1016/j.pnpbp.2006.01.008. Epub 2006 Mar 23. Prog Neuropsychopharmacol Biol Psychiatry. 2006. PMID: 16563589 Free PMC article. Review.
Cited by
-
Post-Traumatic Stress Symptoms Following Childbirth: A Contribution to the Psychometric Evaluation of the Greek Version of the Traumatic Event Scale (TES) (Version B).Healthcare (Basel). 2025 Mar 30;13(7):768. doi: 10.3390/healthcare13070768. Healthcare (Basel). 2025. PMID: 40218065 Free PMC article.
-
Increased antidepressant prescriptions following the 2018 Japan floods: a longitudinal analysis using the national health insurance database.Eur J Psychotraumatol. 2025 Dec;16(1):2537547. doi: 10.1080/20008066.2025.2537547. Epub 2025 Aug 20. Eur J Psychotraumatol. 2025. PMID: 40833291 Free PMC article.
-
Hospitalizations with post-traumatic stress disorder in France between 2013 and 2022: a nationwide retrospective study.Eur Psychiatry. 2025 Jan 15;68(1):e10. doi: 10.1192/j.eurpsy.2024.1810. Eur Psychiatry. 2025. PMID: 39809595 Free PMC article.
-
Epidemiological Profile of Road Traffic Injury Patients in Hospitals in Fako Division, Cameroon: A Foundation for Tailored Post-Traumatic Stress Disorder (PTSD) Management.medRxiv [Preprint]. 2025 Jun 11:2025.06.10.25329319. doi: 10.1101/2025.06.10.25329319. medRxiv. 2025. PMID: 40585159 Free PMC article. Preprint.
-
Exploring metabolomic dynamics in acute stress disorder: amino acids, lipids, and carbohydrates.Front Genet. 2024 Jul 25;15:1394630. doi: 10.3389/fgene.2024.1394630. eCollection 2024. Front Genet. 2024. PMID: 39119583 Free PMC article. Review.
References
-
- Psychiatric Association American . Diagnostic and statistical manual of mental disorders : DSM-5™. Washington DC: American Psychiatric Publishing; 2013.
Publication types
LinkOut - more resources
Full Text Sources