

Comparison of three spot proteinuria measurements for pediatric nephrotic syndrome: based on the International pediatric Nephrology Association 2022 Guidelines
- PMID: 37724557
- PMCID: PMC10512887
- DOI: 10.1080/0886022X.2023.2253324
Comparison of three spot proteinuria measurements for pediatric nephrotic syndrome: based on the International pediatric Nephrology Association 2022 Guidelines
Abstract
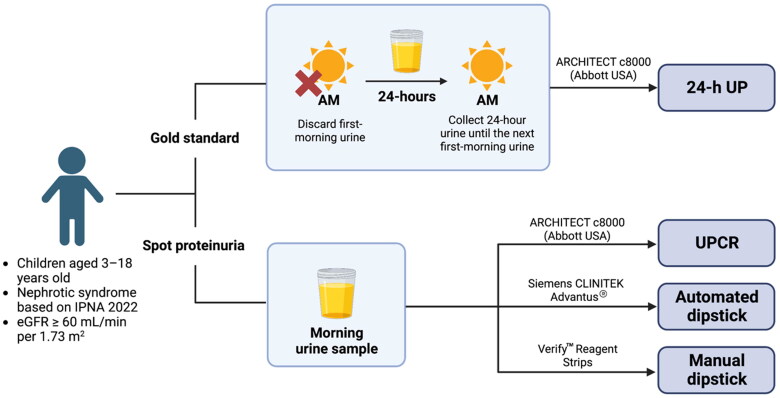
Background: Pediatric nephrotic syndrome (NS) requires routine proteinuria monitoring, which is costly and affects patients' quality of life. The gold-standard 24-h urine protein (UP) measurement is challenging in children, and first-morning urine collection requires specific conditions, making it difficult in outpatient settings. Studies have reported comparability of second or random morning urine sample to the first-morning specimen. This study aimed to compare outcomes of random morning proteinuria measurements to 24-h UP and the roles of the urinary protein creatinine ratio (UPCR) and dipstick tests in pediatric NS, based on International Pediatric Nephrology Association (IPNA) 2022 Guidelines.
Method: Twenty-four-hour and morning urine samples were collected from 92 pediatric NS patients. These were subjected to automated analyses for 24-h UP, UPCR, and semi-automated dipstick analysis. A blinded doctor performed manual dipstick analysis.
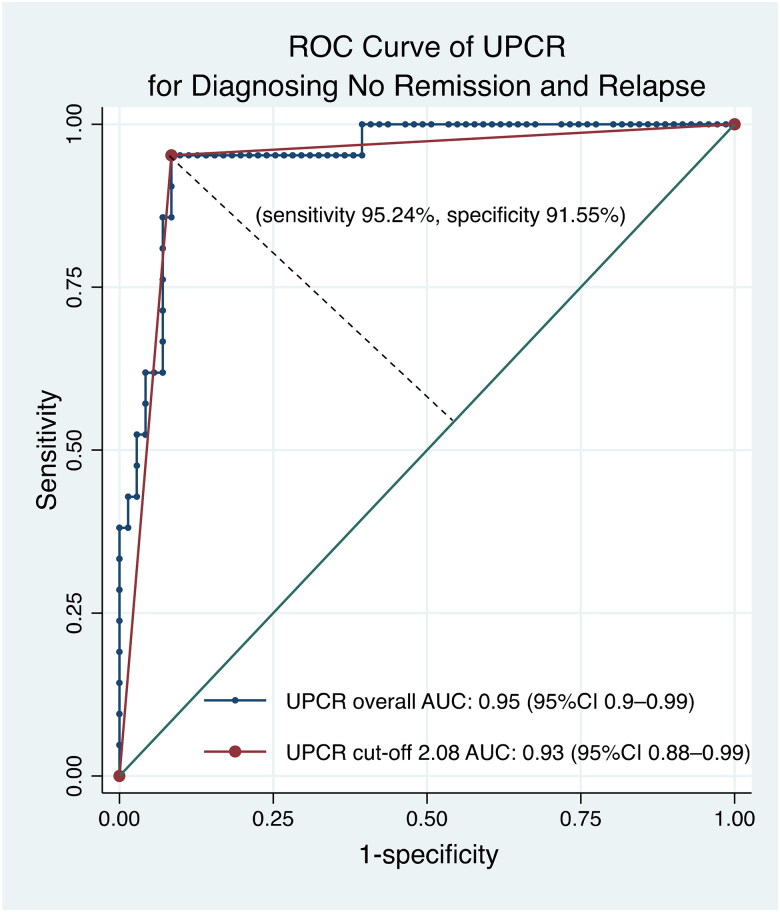
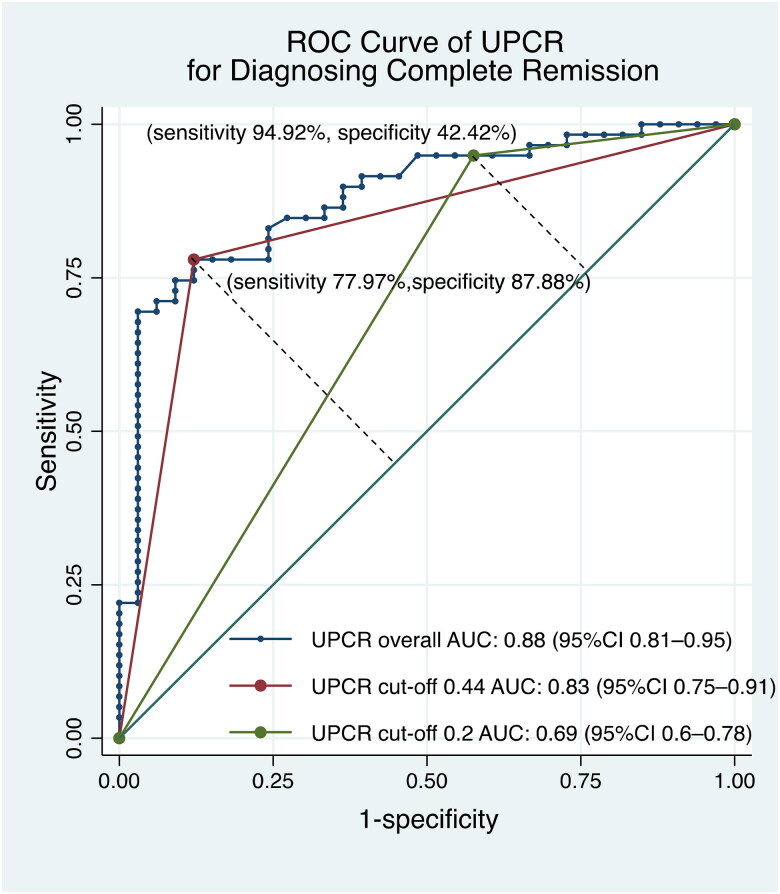
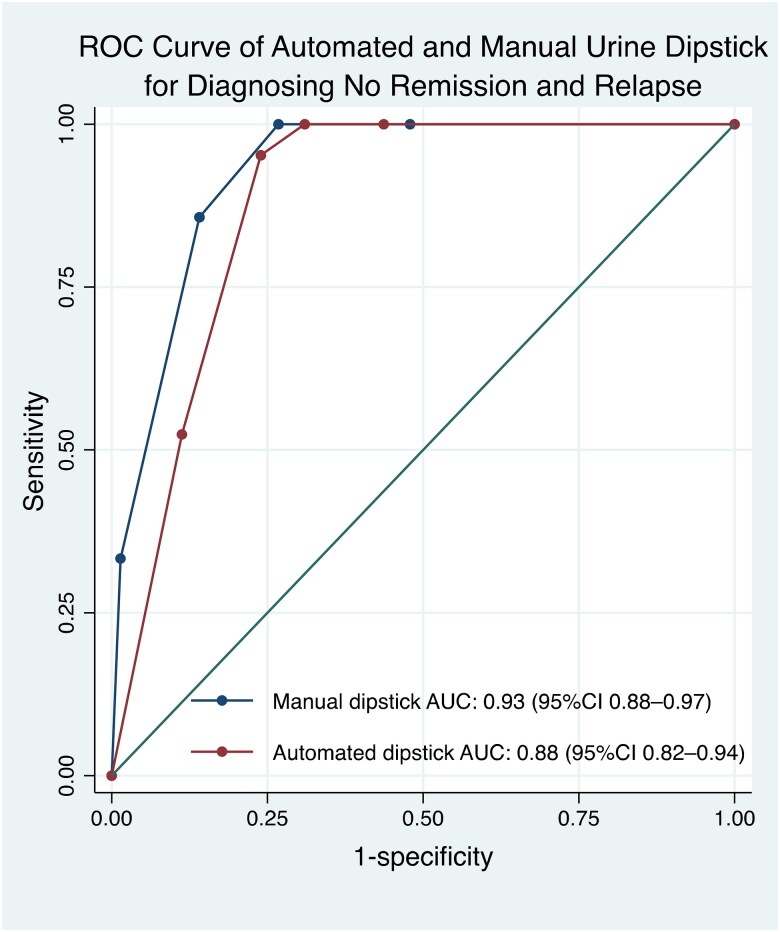
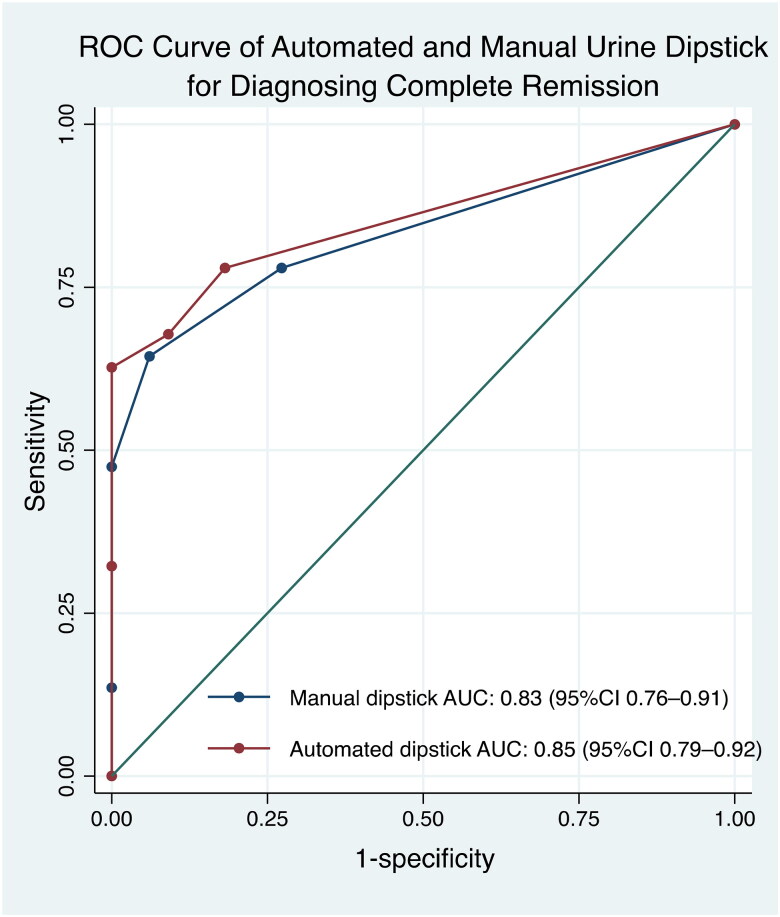
Results: UPCR had a stronger correlation with 24-h UP than with automated and manual urine dipstick tests. UPCR had the highest sensitivity and specificity for predicting no remission/relapse and high sensitivity but low specificity for complete remission. The optimal UPCR cutoff for remission was 0.44 mg/mg and for no remission/relapse was 2.08 mg/mg. Automated and manual dipstick tests demonstrated limited sensitivity but high specificity and similar AUC values for remission/relapse.
Conclusion: UPCR was sensitive and specific for diagnosing no remission/relapse and sensitive but not specific for detecting remission. Manual and automated urine dipstick tests were comparable for remission and no remission/relapse detection. This study supports the IPNA 2022 Guidelines, as 2 mg/mg was the optimal UPCR cutoff for no remission/relapse, while for remission the optimal cutoff was 0.4 mg/mg.
Keywords: Creatinine; relapse; steroid-dependent; steroid-resistant; steroid-sensitive; urine.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
Similar articles
-
Correlation of urine protein/creatinine ratios to 24-h urinary protein for quantitating proteinuria in children.Pediatr Nephrol. 2020 Mar;35(3):463-468. doi: 10.1007/s00467-019-04405-5. Epub 2019 Dec 7. Pediatr Nephrol. 2020. PMID: 31813022
-
A comparison of the utility of the urine dipstick and urine protein-to-creatinine ratio for predicting microalbuminuria in patients with non-diabetic lifestyle-related diseases -a comparison with diabetes.BMC Nephrol. 2022 Nov 24;23(1):377. doi: 10.1186/s12882-022-02974-6. BMC Nephrol. 2022. PMID: 36434544 Free PMC article.
-
Diagnostic efficacy and influence factors of urinary protein/creatinine ratio replacing 24-h urine protein as an evaluator of proteinuria in children.Int Urol Nephrol. 2022 Jun;54(6):1409-1416. doi: 10.1007/s11255-021-03021-3. Epub 2021 Oct 19. Int Urol Nephrol. 2022. PMID: 34668110
-
Diagnostic utility of protein to creatinine ratio (P/C ratio) in spot urine sample within routine clinical practice.Crit Rev Clin Lab Sci. 2020 Aug;57(5):345-364. doi: 10.1080/10408363.2020.1723487. Epub 2020 Feb 14. Crit Rev Clin Lab Sci. 2020. PMID: 32058809 Review.
-
Nephrotic syndrome in infants and children: pathophysiology and management.Paediatr Int Child Health. 2017 Nov;37(4):248-258. doi: 10.1080/20469047.2017.1374003. Epub 2017 Sep 15. Paediatr Int Child Health. 2017. PMID: 28914167 Review.
Cited by
-
Ambulatory blood pressure monitoring in Egyptian children with nephrotic syndrome: single center experience.Ital J Pediatr. 2024 Oct 12;50(1):214. doi: 10.1186/s13052-024-01775-x. Ital J Pediatr. 2024. PMID: 39396026 Free PMC article.
-
Validation and optimization of classification criteria for childhood-onset systemic lupus erythematosus in a multi-center Chinese cohort.Front Immunol. 2025 Jul 17;16:1611349. doi: 10.3389/fimmu.2025.1611349. eCollection 2025. Front Immunol. 2025. PMID: 40746541 Free PMC article.
-
Reliability of the spot urine protein/creatinine ratio for assessing proteinuria in patients with renal disease.J Int Med Res. 2024 Sep;52(9):3000605241281874. doi: 10.1177/03000605241281874. J Int Med Res. 2024. PMID: 39324177 Free PMC article.
-
Perioperative Blood Pressure Management Recommendations in Pediatric Pheochromocytoma: A 10-Year Narrative Review.Kidney Blood Press Res. 2025;50(1):61-82. doi: 10.1159/000542897. Epub 2024 Dec 3. Kidney Blood Press Res. 2025. PMID: 39626645 Free PMC article. Review.
-
Carotid intima-media thickness, fibroblast growth factor 23, and mineral bone disorder in children with chronic kidney disease.BMC Nephrol. 2024 Oct 21;25(1):369. doi: 10.1186/s12882-024-03771-z. BMC Nephrol. 2024. PMID: 39433982 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous