

Technical Feasibility of Quantitative Measurement of Various Degrees of Small Bowel Motility Using Cine Magnetic Resonance Imaging
- PMID: 37724587
- PMCID: PMC10613842
- DOI: 10.3348/kjr.2023.0144
Technical Feasibility of Quantitative Measurement of Various Degrees of Small Bowel Motility Using Cine Magnetic Resonance Imaging
Abstract
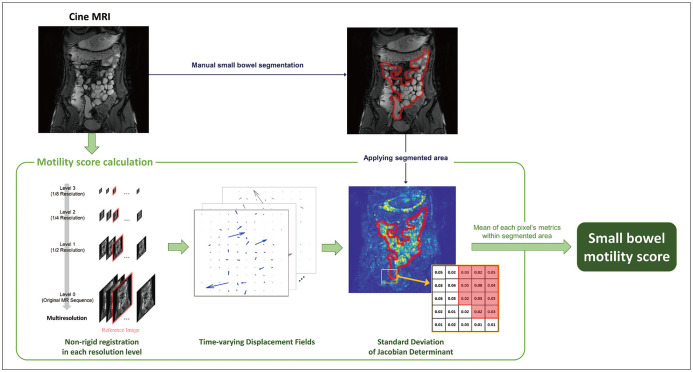
Objective: Cine magnetic resonance imaging (MRI) has emerged as a noninvasive method to quantitatively assess bowel motility. However, its accuracy in measuring various degrees of small bowel motility has not been extensively evaluated. We aimed to draw a quantitative small bowel motility score from cine MRI and evaluate its performance in a population with varying degrees of small bowel motility.
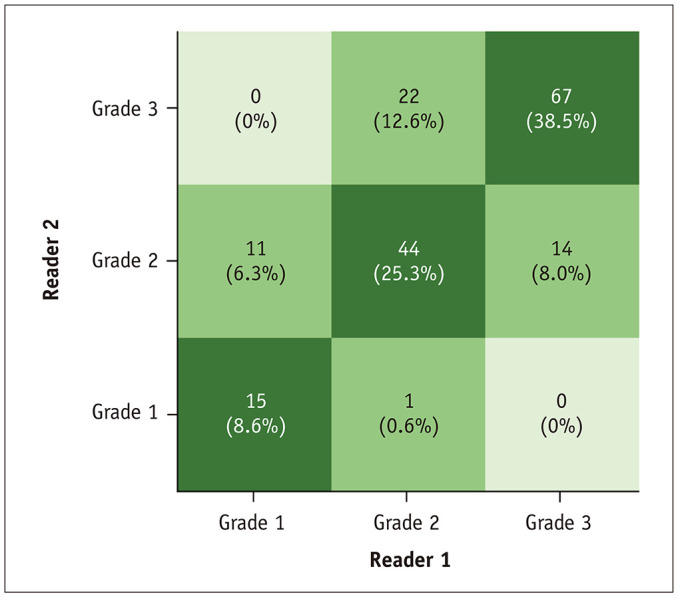
Materials and methods: A total of 174 participants (28.5 ± 7.6 years; 135 males) underwent a 22-second-long cine MRI sequence (2-dimensional balanced turbo-field echo; 0.5 seconds per image) approximately 5 minutes after being intravenously administered 10 mg of scopolamine-N-butyl bromide to deliberately create diverse degrees of small bowel motility. In a manually segmented area of the small bowel, motility was automatically quantified using a nonrigid registration and calculated as a quantitative motility score. The mean value (MV) of motility grades visually assessed by two radiologists was used as a reference standard. The quantitative motility score's correlation (Spearman's ρ) with the reference standard and performance (area under the receiver operating characteristics curve [AUROC], sensitivity, and specificity) for diagnosing adynamic small bowel (MV of 1) were evaluated.
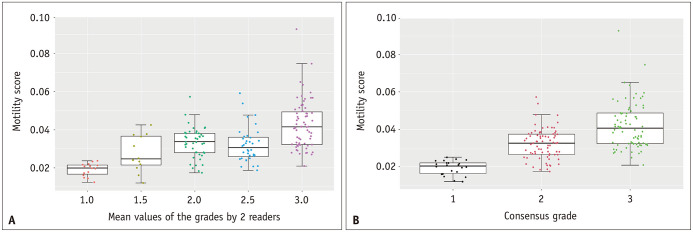
Results: For the MV of the quantitative motility scores at grades 1, 1.5, 2, 2.5, and 3, the mean ± standard deviation values were 0.019 ± 0.003, 0.027 ± 0.010, 0.033 ± 0.008, 0.032 ± 0.009, and 0.043 ± 0.013, respectively. There was a significant positive correlation between the quantitative motility score and the MV (ρ = 0.531, P < 0.001). The AUROC value for diagnosing a MV of 1 (i.e., adynamic small bowel) was 0.953 (95% confidence interval, 0.923-0.984). Moreover, the optimal cutoff for the quantitative motility score was 0.024, with a sensitivity of 100% (15/15) and specificity of 89.9% (143/159).
Conclusion: The quantitative motility score calculated from a cine MRI enables diagnosis of an adynamic small bowel, and potentially discerns various degrees of bowel motility.
Keywords: Bowel; Cine imaging; Gastrointestinal motility; Magnetic resonance imaging; Small intestine.
Copyright © 2023 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Husebye E. The patterns of small bowel motility: physiology and implications in organic disease and functional disorders. Neurogastroenterol Motil. 1999;11:141–161. - PubMed
-
- Soffer EE. Small bowel motility: ready for prime time? Curr Gastroenterol Rep. 2000;2:364–369. - PubMed
-
- Kellow JE, Phillips SF. Altered small bowel motility in irritable bowel syndrome is correlated with symptoms. Gastroenterology. 1987;92:1885–1893. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
