

Nomogram based on clinical characteristics and radiological features for the preoperative prediction of spread through air spaces in patients with clinical stage IA non-small cell lung cancer: a multicenter study
- PMID: 37724737
- PMCID: PMC10679558
- DOI: 10.4274/dir.2023.232404
Nomogram based on clinical characteristics and radiological features for the preoperative prediction of spread through air spaces in patients with clinical stage IA non-small cell lung cancer: a multicenter study
Abstract
Purpose: To investigate the value of clinical characteristics and radiological features for predicting spread through air spaces (STAS) in patients with clinical stage IA non-small cell lung cancer (NSCLC).
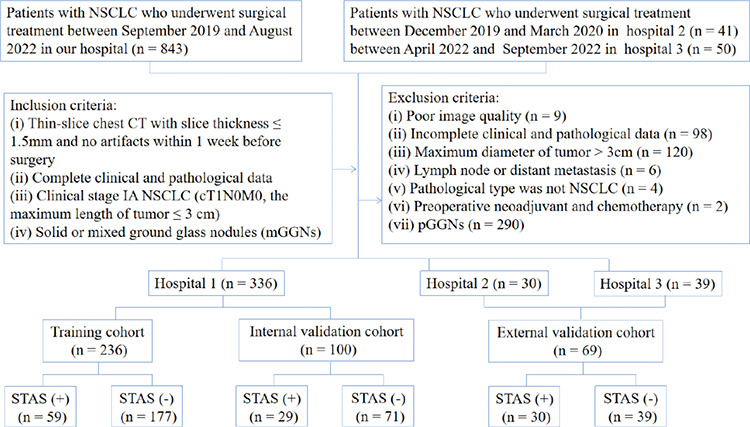
Methods: A total of 336 patients with NSCLC from our hospital were randomly divided into two groups, i.e., the training cohort (n = 236) and the internal validation cohort (n = 100) (7:3 ratio). Furthermore, 69 patients from two other hospitals were collected as the external validation cohort. Eight clinical patient characteristics were recorded, and 20 tumor radiological features were quantitatively measured and qualitatively analyzed. In the training cohort, the differences in clinical characteristics and radiological features were compared using univariate and multivariate analysis. A nomogram was created, and the predictive efficacy of the model was evaluated in the validation cohorts. The receiver operating characteristic curve and area under the curve (AUC) value were used to evaluate the discriminative ability of the model. In addition, the Hosmer-Lemeshow test and calibration curve were used to evaluate the goodness-of-fit of the model, and the decision curve was used to analyze the model's clinical application value.
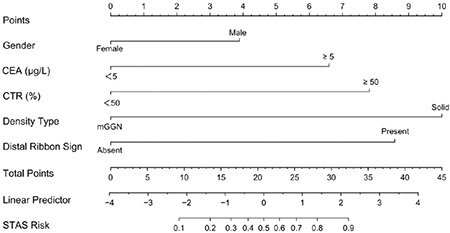
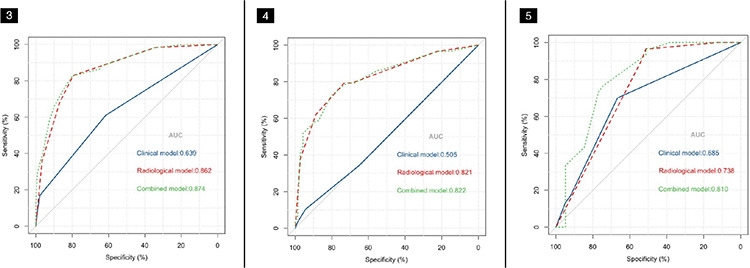
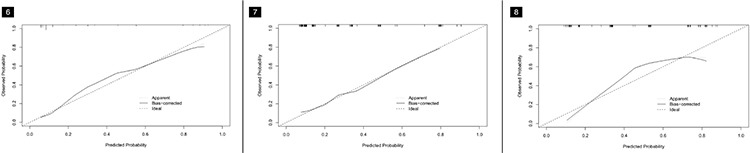
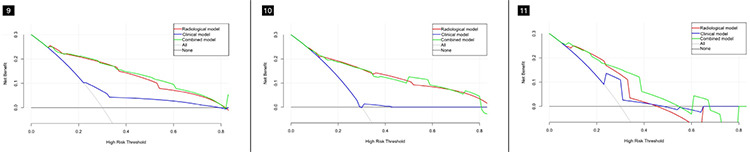
Results: The best predictors included gender, the carcinoembryonic antigen (CEA), consolidation-to-tumor ratio (CTR), density type, and distal ribbon sign. Among these, the tumor density type [odds ratio (OR): 6.738] and distal ribbon sign (OR: 5.141) were independent risk factors for predicting the STAS status. Moreover, three different STAS prediction models were constructed, i.e., a clinical, radiological, and combined model. The clinical model comprised gender and the CEA, the radiological model included the CTR, density type, and distal ribbon sign, and the combined model comprised the above two models. A DeLong test results revealed that the combined model was superior to the clinical model in all three cohorts and superior to the radiological model in the external validation cohort; the cohort AUC values were 0.874, 0.822, and 0.810, respectively. The results also showed that the combined model had the highest diagnostic efficacy among the models. The Hosmer-Lemeshow test showed that the combined model showed a good fit in all three cohorts, and the calibration curve showed that the predicted probability value of the combined model was in good agreement with the actual STAS status. Finally, the decision curve showed that the combined model had a better clinical application value than the clinical and radiological models.
Conclusion: The nomogram created in this study, based on clinical characteristics and radiological features, has a high diagnostic efficiency for predicting the STAS status in patients with clinical stage IA NSCLC and may support the creation of personalized treatment strategies before surgery.
Keywords: Spread through air spaces; nomogram; non-small cell lung cancer; prediction; radiological.
Conflict of interest statement
The authors declared no conflicts of interest.
This research was funded by the National Key R&D Program of China (2022YFC2010000, 2022YFC2010002), the Key Program of National Natural Science Foundation of China (81930049), the National Natural Science Foundation of China (82171926, 82202140), the Shanghai Sailing Program (20YF1449000), the Shanghai Science and Technology Innovation Action Plan Program (19411951300), the Clinical Innovative Project of Shanghai Changzheng Hospital (2020YLCYJ-Y24), and the Program of Science and Technology Commission of Shanghai Municipality (21DZ2202600).
Figures
Similar articles
-
A narrative review of preoperative CT for predicting spread through air spaces of lung cancer.Transl Lung Cancer Res. 2025 Apr 30;14(4):1471-1481. doi: 10.21037/tlcr-24-952. Epub 2025 Apr 27. Transl Lung Cancer Res. 2025. PMID: 40386727 Free PMC article. Review.
-
Preoperative nomogram for predicting spread through air spaces in clinical-stage IA non-small cell lung cancer using 18F-fluorodeoxyglucose positron emission tomography/computed tomography.J Cancer Res Clin Oncol. 2024 Apr 10;150(4):185. doi: 10.1007/s00432-024-05674-w. J Cancer Res Clin Oncol. 2024. PMID: 38598007 Free PMC article.
-
Nomogram model for the preoperative prediction of spread through air spaces in sub-centimeter non-small cell lung cancer.J Cardiothorac Surg. 2025 Apr 23;20(1):218. doi: 10.1186/s13019-025-03441-7. J Cardiothorac Surg. 2025. PMID: 40264135 Free PMC article.
-
CT-Based Intratumoral and Peritumoral Radiomics Nomograms for the Preoperative Prediction of Spread Through Air Spaces in Clinical Stage IA Non-small Cell Lung Cancer.J Imaging Inform Med. 2024 Apr;37(2):520-535. doi: 10.1007/s10278-023-00939-1. Epub 2024 Jan 10. J Imaging Inform Med. 2024. PMID: 38343212 Free PMC article.
-
Pretreatment prediction of tumour spread through air spaces in clinical stage I non-small-cell lung cancer.Eur J Cardiothorac Surg. 2022 Aug 3;62(3):ezac248. doi: 10.1093/ejcts/ezac248. Eur J Cardiothorac Surg. 2022. PMID: 35385066 Free PMC article.
Cited by
-
A narrative review of preoperative CT for predicting spread through air spaces of lung cancer.Transl Lung Cancer Res. 2025 Apr 30;14(4):1471-1481. doi: 10.21037/tlcr-24-952. Epub 2025 Apr 27. Transl Lung Cancer Res. 2025. PMID: 40386727 Free PMC article. Review.
-
Clinical, pathological, and computed tomography morphological features of lung cancer with spread through air spaces.Transl Lung Cancer Res. 2024 Oct 31;13(10):2802-2812. doi: 10.21037/tlcr-24-715. Epub 2024 Oct 21. Transl Lung Cancer Res. 2024. PMID: 39507029 Free PMC article.
-
Improving prediction accuracy of spread through air spaces in clinical-stage T1N0 lung adenocarcinoma using computed tomography imaging models.JTCVS Open. 2024 Aug 17;21:290-303. doi: 10.1016/j.xjon.2024.07.018. eCollection 2024 Oct. JTCVS Open. 2024. PMID: 39534334 Free PMC article.
-
A Bayesian deep learning model with consolidation-to-tumor ratio (CTR) prior revolutionizes the prediction of spread through air spaces (STAS) in stage IA lung adenocarcinoma: a large-scale diagnostic study.Transl Lung Cancer Res. 2025 May 30;14(5):1516-1530. doi: 10.21037/tlcr-24-890. Epub 2025 May 27. Transl Lung Cancer Res. 2025. PMID: 40535077 Free PMC article.
-
A nomogram integrating the clinical and CT imaging characteristics for assessing spread through air spaces in clinical stage IA lung adenocarcinoma.Front Immunol. 2025 Apr 11;16:1519766. doi: 10.3389/fimmu.2025.1519766. eCollection 2025. Front Immunol. 2025. PMID: 40292286 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. - PubMed
-
- Ettinger DS, Wood DE, Aisner DL, et al. NCCN Guidelines® Insights: non-small cell lung cancer, version 2 2023. J Natl Compr Canc Netw. 2023;21(4):340–350. - PubMed
-
- Saji H, Okada M, Tsuboi M, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet. 2022;399(10335):1607–1617. - PubMed
-
- Suzuki K, Saji H, Aokage K, et al. Comparison of pulmonary segmentectomy and lobectomy: safety results of a randomized trial. J Thorac Cardiovasc Surg. 2019;158(3):895–907. - PubMed
-
- Suzuki K, Watanabe SI, Wakabayashi M, et al. A single-arm study of sublobar resection for ground-glass opacity dominant peripheral lung cancer. J Thorac Cardiovasc Surg. 2022;163(1):289–301. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
