

Digital Health Implementation Strategies Coproduced With Adults With Acquired Brain Injury, Their Close Others, and Clinicians: Mixed Methods Study With Collaborative Autoethnography and Network Analysis
- PMID: 37725413
- PMCID: PMC10548320
- DOI: 10.2196/46396
Digital Health Implementation Strategies Coproduced With Adults With Acquired Brain Injury, Their Close Others, and Clinicians: Mixed Methods Study With Collaborative Autoethnography and Network Analysis
Abstract
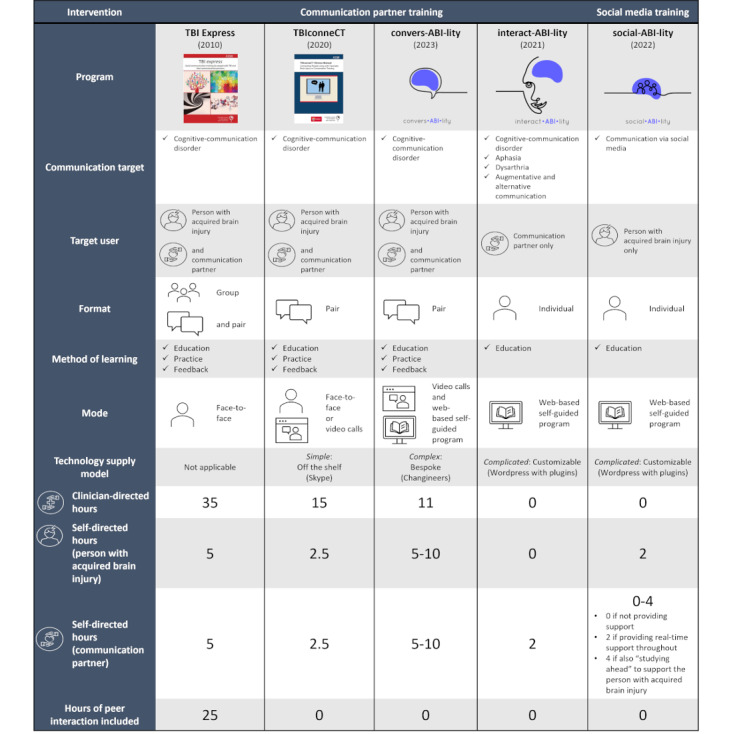
Background: Acquired brain injuries (ABIs), such as stroke and traumatic brain injury, commonly cause cognitive-communication disorders, in which underlying cognitive difficulties also impair communication. As communication is an exchange with others, close others such as family and friends also experience the impact of cognitive-communication impairment. It is therefore an internationally recommended best practice for speech-language pathologists to provide communication support to both people with ABI and the people who communicate with them. Current research also identifies a need for neurorehabilitation professionals to support digital communication, such as social media use, after ABI. However, with >135 million people worldwide affected by ABI, alternate and supplementary service delivery models are needed to meet these communication needs. The "Social Brain Toolkit" is a novel suite of 3 interventions to deliver communication rehabilitation via the internet. However, digital health implementation is complex, and minimal guidance exists for ABI.
Objective: This study aimed to support the implementation of the Social Brain Toolkit by coproducing implementation knowledge with people with ABI, people who communicate with people with ABI, clinicians, and leaders in digital health implementation.
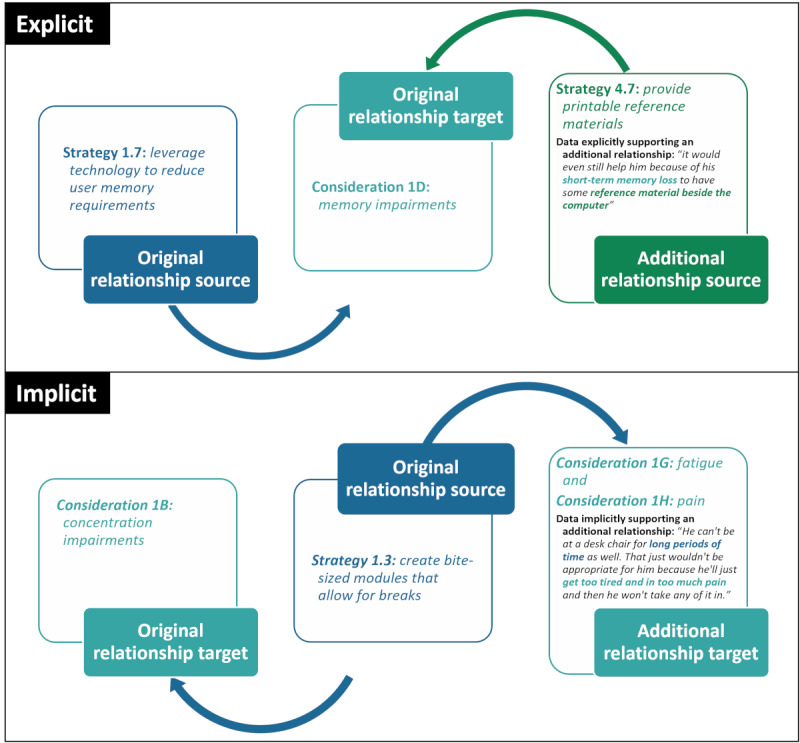
Methods: A maximum variation sample (N=35) of individuals with living experience of ABI, close others, clinicians, and digital health implementation leaders participated in an explanatory sequential mixed methods design. Stakeholders quantitatively prioritized 4 of the 7 theoretical domains of the Nonadoption, Abandonment, Scale-up, Spread, and Sustainability (NASSS) framework as being the most important for Social Brain Toolkit implementation. Qualitative interview and focus group data collection focused on these 4 domains. Data were deductively analyzed against the NASSS framework with stakeholder coauthors to determine implementation considerations and strategies. A collaborative autoethnography of the research was conducted. Interrelationships between considerations and strategies were identified through a post hoc network analysis.
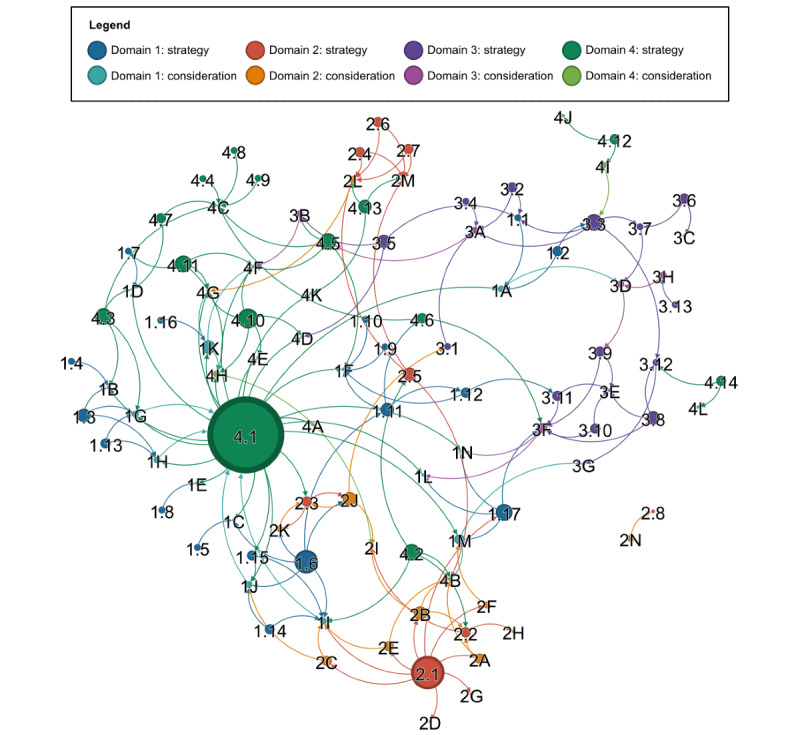
Results: Across the 4 prioritized domains of "condition," "technology," "value proposition," and "adopters," 48 digital health implementation considerations and 52 tailored developer and clinician implementation strategies were generated. Benefits and challenges of coproduction were identified. The post hoc network analysis revealed 172 unique relationships between the identified implementation considerations and strategies, with user and persona testing and responsive design identified as the potentially most impactful strategies.
Conclusions: People with ABI, close others, clinicians, and digital health leaders coproduced new knowledge of digital health implementation considerations for adults with ABI and the people who communicate with them, as well as tailored implementation strategies. Complexity-informed network analyses offered a data-driven method to identify the 2 most potentially impactful strategies. Although the study was limited by a focus on 4 NASSS domains and the underrepresentation of certain demographics, the wealth of actionable implementation knowledge produced supports future coproduction of implementation research with mutually beneficial outcomes for stakeholders and researchers.
International registered report identifier (irrid): RR2-10.2196/35080.
Keywords: brain injury; caregivers; complexity; delivery of health care; digital health; implementation science; internet interventions; mobile phone; psychosocial; psychosocial interventions; stroke; traumatic brain injury.
©Melissa Miao, Rosemary Morrow, Alexander Salomon, Ben Mcculloch, Jean-Christophe Evain, Meg Rebecca Wright, Marie Therese Murphy, Monica Welsh, Liz Williams, Emma Power, Rachael Rietdijk, Deborah Debono, Melissa Brunner, Leanne Togher. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 19.09.2023.
Conflict of interest statement
Conflicts of Interest: MM, EP, RR, MB, and LT are developers of the Social Brain Toolkit in collaboration with end users, with no other conflicts declared. All other authors declare no other conflicts of interest.
Figures
Similar articles
-
Coproducing Knowledge of the Implementation of Complex Digital Health Interventions for Adults with Acquired Brain Injury and their Communication Partners: Protocol for a Mixed Methods Study.JMIR Res Protoc. 2022 Jan 10;11(1):e35080. doi: 10.2196/35080. JMIR Res Protoc. 2022. PMID: 35006082 Free PMC article.
-
A Web-Based Service Delivery Model for Communication Training After Brain Injury: Protocol for a Mixed Methods, Prospective, Hybrid Type 2 Implementation-Effectiveness Study.JMIR Res Protoc. 2021 Dec 9;10(12):e31995. doi: 10.2196/31995. JMIR Res Protoc. 2021. PMID: 34889770 Free PMC article.
-
Developing a Digital Health Intervention for Conversation Skills After Brain Injury (convers-ABI-lity) Using a Collaborative Approach: Mixed Methods Study.J Med Internet Res. 2023 Aug 9;25:e45240. doi: 10.2196/45240. J Med Internet Res. 2023. PMID: 37556179 Free PMC article.
-
Developing Social-ABI-lity: An Online Course to Support Safe Use of Social Media for Connection After Acquired Brain Injury.Am J Speech Lang Pathol. 2023 Mar 23;32(2S):924-940. doi: 10.1044/2022_AJSLP-22-00099. Epub 2022 Dec 9. Am J Speech Lang Pathol. 2023. PMID: 36492293 Review.
-
The effects of choral singing on communication impairments in acquired brain injury: A systematic review.Int J Lang Commun Disord. 2020 May;55(3):303-319. doi: 10.1111/1460-6984.12527. Epub 2020 Feb 25. Int J Lang Commun Disord. 2020. PMID: 32096327
Cited by
-
The Significance of a Cerebrovascular Accident Outcome Prediction Model for Patients, Family Members, and Health Care Professionals: Qualitative Evaluation Study.JMIR Hum Factors. 2025 Jan 22;12:e56521. doi: 10.2196/56521. JMIR Hum Factors. 2025. PMID: 39842003 Free PMC article.
References
-
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 Dec;396(10267):2006–17. doi: 10.1016/s0140-6736(20)32340-0. - DOI - PMC - PubMed
-
- GBD 2016 Neurology Collaborators Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019 May;18(5):459–80. doi: 10.1016/S1474-4422(18)30499-X. https://linkinghub.elsevier.com/retrieve/pii/S1474-4422(18)30499-X S1474-4422(18)30499-X - DOI - PMC - PubMed
-
- GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019 Jan;18(1):56–87. doi: 10.1016/S1474-4422(18)30415-0. https://linkinghub.elsevier.com/retrieve/pii/S1474-4422(18)30415-0 S1474-4422(18)30415-0 - DOI - PMC - PubMed
-
- Norman RS, Swan AA, Jenkins A, Ballard M, Amuan M, Pugh MJ. Updating and refining prevalence rates of traumatic brain injury–related communication disorders among post-9/11 veterans: a chronic effects of neurotrauma consortium study. Perspect ASHA SIGs. 2021 Oct 20;6(5):1060–72. doi: 10.1044/2020_persp-20-00011. - DOI
-
- Togher L, Douglas J, Turkstra LS, Welch-West P, Janzen S, Harnett A, Kennedy M, Kua A, Patsakos E, Ponsford J, Teasell R, Bayley MT, Wiseman-Hakes C. INCOG 2.0 Guidelines for cognitive rehabilitation following traumatic brain injury, part IV: cognitive-communication and social cognition disorders. J Head Trauma Rehabil. 2023;38(1):65–82. doi: 10.1097/HTR.0000000000000835. https://digitalcommons.chapman.edu/comm_science_articles/26/ 00001199-202301000-00006 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
