

In-class transition (iCT) of proteasome inhibitor-based therapy: a community approach to multiple myeloma management
- PMID: 37726298
- PMCID: PMC10509188
- DOI: 10.1038/s41408-023-00912-9
In-class transition (iCT) of proteasome inhibitor-based therapy: a community approach to multiple myeloma management
Abstract
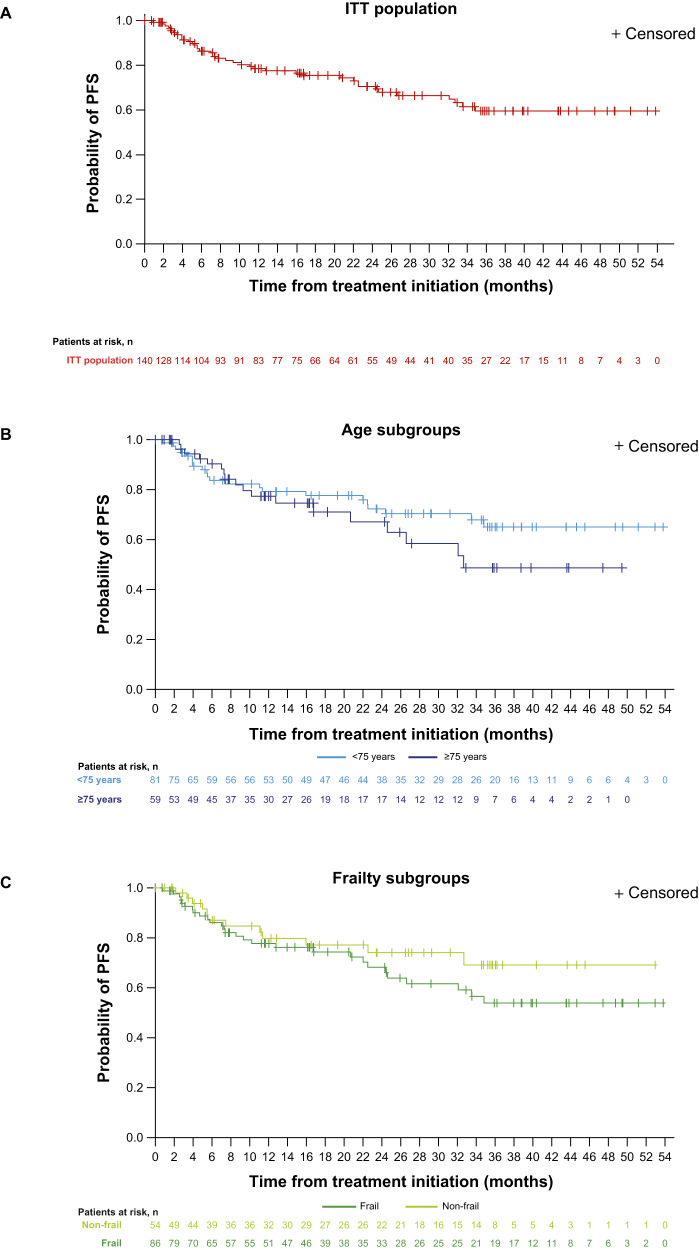
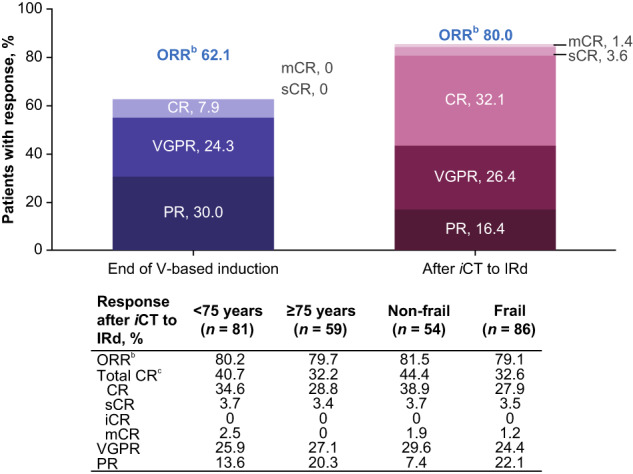
Long-term proteasome inhibitor (PI) treatment can improve multiple myeloma (MM) outcomes, but this can be difficult to achieve in clinical practice due to toxicity, comorbidities, and the burden of repeated parenteral administration. US MM-6 (NCT03173092) enrolled transplant-ineligible patients with newly diagnosed MM to receive all-oral ixazomib-lenalidomide-dexamethasone (IRd; ≤39 cycles or until progression or toxicity) following three cycles of bortezomib-based induction. Primary endpoint: 2-year progression-free survival (PFS). Key secondary/exploratory endpoints included overall response rate (ORR), overall survival (OS), safety, quality of life (QoL), treatment satisfaction, and actigraphy. At datacut, in the fully accrued cohort of 140 patients, median age was 73 years with 42% aged ≥75 and 61% deemed frail; 10% of patients were ongoing on treatment. After a median follow-up of 27 months, the 2-year PFS rate was 71% (95% confidence interval: 61-78). ORR increased from 62% at the end of induction to 80% following in-class transition (iCT) to IRd for a median of 11 months. The 2-year OS rate was 86%. The overall safety profile/actigraphy levels were consistent with previous reports; QoL/treatment satisfaction scores were stable with ongoing therapy. iCT to IRd may allow prolonged PI-based therapy with promising efficacy and a tolerable safety profile, while maintaining QoL.
© 2023. Springer Nature Limited.
Conflict of interest statement
RMR: Member of board of directors/advisory committee: Amgen, Bristol Myers Squibb (Celgene), Coherus, Fresenius-Kabi, Sanofi, Takeda, and Karyopharm; Current employee and equity holder: McKesson. SKG: Honoraria: BMS, Genentech, and GSK; Speakers bureau: BMS, Celgene, GSK, Takeda, and Beigene; Member of board of directors/advisory committee: Takeda. SJN: Current employee: Takeda. REB: Consultancy: Alexion, AbbVie, Novartis, Janssen, Pharmacyclics, and Puma; Honoraria: AbbVie, Novartis, Bayer, Seattle Genetics, Coheris, Kyte Pharma, Celgene, Helsin, and Amgen; Research funding: Puma, Takeda, and Incyte; Speakers bureau: Novartis, Janssen, Pharmacyclics, Puma, Takeda, Incyte, Amgen, Pfizer, BMS, Tessaro, AstraZeneca, Genomic Health, Sanofi, Clovis, Exelexis, and Lilly. SK: nothing to disclose. S.M.: Honoraria: Morphosys; Current equity holder: Genmab. RML: nothing to disclose. HAY: Speakers bureau: Karyopharm, AstraZeneca, Janssen, Beigene, GSK, Sanofi, Amgen, Pharmacyclics, and Takeda; Current stockholder: Karyopharm; Current employee: Texas Oncology. DC: Current employee: Takeda; Ownership of stock/shares with Takeda. EL: Current employee: Takeda. PW: Current employee: Takeda. JR: Consulting fees from Takeda and BMS/Celgene.
Figures

References
-
- Mateos MV, Richardson PG, Dimopoulos MA, Palumbo A, Anderson KC, Shi H, et al. Effect of cumulative bortezomib dose on survival in multiple myeloma patients receiving bortezomib-melphalan-prednisone in the phase III VISTA study. Am J Hematol. 2015;90:314–9. - PubMed
-
- Jimenez-Zepeda VH, Duggan P, Neri P, Tay J, Bahlis NJ. Bortezomib-containing regimens (BCR) for the treatment of non-transplant eligible multiple myeloma. Ann Hematol. 2017;96:431–9. - PubMed
-
- Durie BG, Hoering A, Abidi MH, Rajkumar SV, Epstein J, Kahanic SP, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial. Lancet. 2017;389:519–27. - PMC - PubMed
-
- San Miguel JF, Schlag R, Khuageva NK, Dimopoulos MA, Shpilberg O, Kropff M, et al. Bortezomib plus melphalan and prednisone for initial treatment of multiple myeloma. New Engl J Med. 2008;359:906–17. - PubMed
-
- San Miguel JF, Schlag R, Khuageva NK, Dimopoulos MA, Shpilberg O, Kropff M, et al. Persistent overall survival benefit and no increased risk of second malignancies with bortezomib-melphalan-prednisone versus melphalan-prednisone in patients with previously untreated multiple myeloma. J Clin Oncol. 2012;31:448–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
