

New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: a study of 14 upper anterior teeth
- PMID: 37726360
- PMCID: PMC10509208
- DOI: 10.1038/s41598-023-42767-x
New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: a study of 14 upper anterior teeth
Abstract
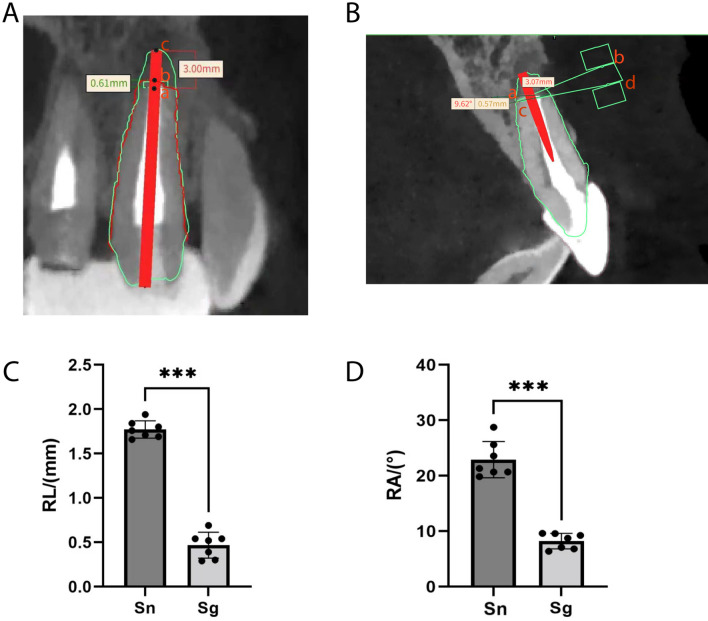
We aimed to design a novel three-dimensional (3D) printed surgical guide and evaluate its accuracy in assisting endodontic microsurgeries. A new 3D printed surgical guide was designed by computer-aided design and computer-aided manufacturing (CAD/CAM) technology and applied to 7 patients who underwent endodontic microsurgeries of upper anterior teeth from 2020.01 to 2020.12 as the experimental group. 7 patients who suffered from endodontic microsurgeries operated by the same surgeon without using the surgical guide from 2019.01 to 2019.12 were selected as the control group. Cone beam computed tomography (CBCT) was performed more than 12 months after operation, and the accuracy of apical resection was compared between the two groups. The accuracy of the microsurgery focused on the length and angle of the root apical resection. In the study, CBCT data and oral digital scanning data were used to reconstruct 3D models of periapical lesions with soft and hard tissue information, based on which we designed the new 3D printed surgical guides. The guides were successfully applied to the apectomy in endodontic microsurgeries. The deviation of the apical resection length of the experimental group (0.467 ± 0.146 mm) was better than that of the control group (1.743 ± 0.122 mm) (P < 0.0001), and the deviation of the apical resection angle of the experimental group (9.711 ± 3.593°) was significantly less than that of the control group (22.400 ± 3.362°) (P < 0.0001). The 3D-printed surgical guide could effectively guide endodontic microsurgery and improve its accuracy by fixing both the position and the angle of apectomy. The new type of surgical guide could accurately localize the root apex and guide the apical resection.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
