

Trimester-specific reference intervals for hemoglobin A1c in non-diabetic pregnancy in a Chinese population
- PMID: 37726666
- PMCID: PMC10507880
- DOI: 10.1186/s12884-023-05980-0
Trimester-specific reference intervals for hemoglobin A1c in non-diabetic pregnancy in a Chinese population
Abstract
Background: Physiological glycated hemoglobin (HbA1c) values in each trimester are not well defined. This study aimed to determine trimester-specific reference intervals for HbA1c levels in non-diabetic pregnant women in China.
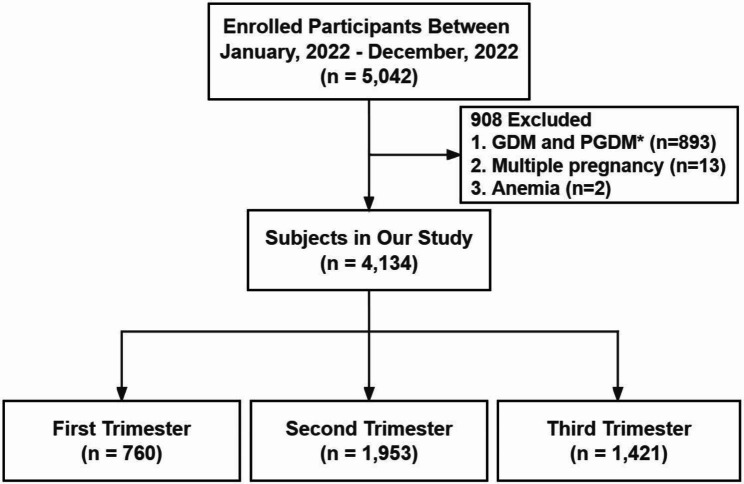
Methods: In this cross-sectional study, 5,042 Chinese pregnant women from 6 to 41 weeks of gestation were screened. An inclusion of 4,134 non-diabetic women was made to determine the reference intervals, they were divided into three trimesters: trimester 1 (T1), 6 weeks to 13 weeks + 6 days, trimester 2 (T2), 14 weeks to 27 weeks + 6 days, and trimester 3 (T3), 28 weeks to 41 weeks + 6 days. A total of 4,134 women (T1 n = 760, T2 n = 1,953, and T3 n = 1,421) provided blood samples which were analyzed for HbA1c concentrations. HbA1c was measured using high-performance liquid chromatography. The median and percentile (2.5th to 97.5th) for the HbA1c reference intervals were calculated for each trimester.
Results: In total, 8,732 HbA1c measurements were taken. Reference intervals for HbA1c expressed as median and percentile (2.5th to 97.5th) for each trimester were: T1: 4.7 (4.0-5.5%), T2: 4.5 (3.9-5.3%), and T3: 4.8 (4.1-5.7%) respectively. The HbA1c levels were significantly lower in the second trimester compared to those in the first trimester (p < 0.0001), and higher in the third trimester compared to the second trimester (p < 0.0001).
Conclusions: The reference intervals for HbA1c levels were 3.9-5.7% with upper limits of 5.5% in the first trimester, 5.3% in the second trimester, and 5.7% in the third trimester. These findings highlight the importance of considering trimester-specific reference intervals for HbA1c in non-diabetic pregnant women to promote maternal and fetal health.
Keywords: Glycated hemoglobin; Non-diabetic; Pregnancy; Reference intervals.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
