

Immunologic constant of rejection as a predictive biomarker of immune checkpoint inhibitors efficacy in non-small cell lung cancer
- PMID: 37726776
- PMCID: PMC10507965
- DOI: 10.1186/s12967-023-04463-2
Immunologic constant of rejection as a predictive biomarker of immune checkpoint inhibitors efficacy in non-small cell lung cancer
Abstract
Background: Anti-PD1/PDL1 immune checkpoint inhibitors (ICI) transformed the prognosis of patients with advanced non-small cell lung cancer (NSCLC). However, the response rate remains disappointing and toxicity may be life-threatening, making urgent identification of biomarkers predictive for efficacy. Immunologic Constant of Rejection signature (ICR) is a 20-gene expression signature of cytotoxic immune response with prognostic value in some solid cancers. Our objective was to assess its predictive value for benefit from anti-PD1/PDL1 in patients with advanced NSCLC.
Methods: We retrospectively profiled 44 primary tumors derived from NSCLC patients treated with ICI as single-agent in at least the second-line metastatic setting. Transcriptomic analysis was performed using the nCounter® analysis system and the PanCancer Immune Profiling Panel. We then pooled our data with clinico-biological data from four public gene expression data sets, leading to a total of 162 NSCLC patients treated with single-agent anti-PD1/PDL1. ICR was applied to all samples and correlation was searched between ICR classes and the Durable Clinical Benefit (DCB), defined as stable disease or objective response according to RECIST 1.1 for a minimum of 6 months after the start of ICI.
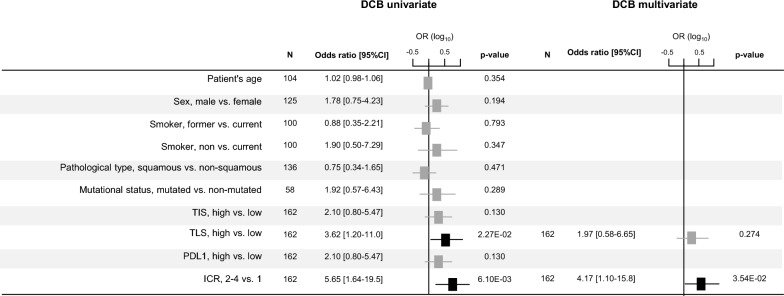
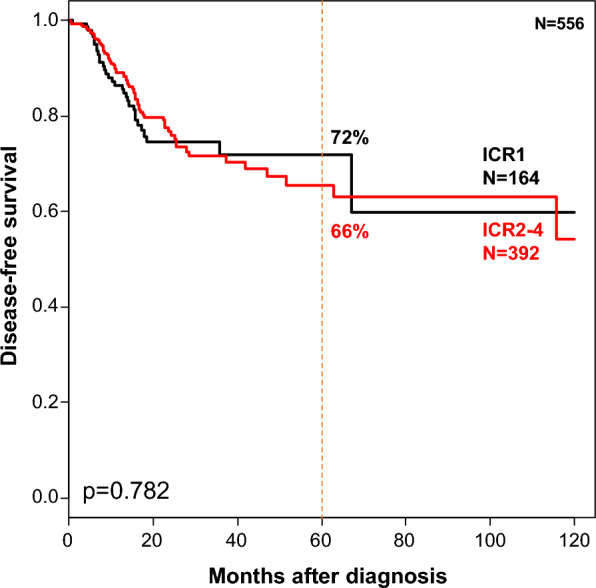
Results: The DCB rate was 29%; 22% of samples were classified as ICR1, 30% ICR2, 22% ICR3, and 26% ICR4. These classes were not associated with the clinico-pathological variables, but showed enrichment from ICR1 to ICR4 in quantitative/qualitative markers of immune response. ICR2-4 class was associated with a 5.65-fold DCB rate when compared with ICR1 class. In multivariate analysis, ICR classification remained associated with DCB, independently from PDL1 expression and other predictive immune signatures. By contrast, it was not associated with disease-free survival in 556 NSCLC TCGA patients untreated with ICI.
Conclusion: The 20-gene ICR signature was independently associated with benefit from anti-PD1/PDL1 ICI in patients with advanced NSCLC. Validation in larger retrospective and prospective series is warranted.
Keywords: Biomarkers; ICR signature; Immune checkpoints inhibitors; Immune therapy; Lung cancer; Transcriptomics.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
A Mogenet received consulting fees from Takeda, Viatris and Pfizer and travel fees from BMS and Pfizer. The other authors have declared no competing interests.
Figures

References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. - PubMed
-
- Tan AC, Tan DSW. Targeted therapies for lung cancer patients with oncogenic driver molecular alterations. J Clin Oncol. 2022;40(6):611–625. - PubMed
-
- Miller JFAP, Sadelain M. The journey from discoveries in fundamental immunology to cancer immunotherapy. Cancer Cell. 2015;27(4):439–449. - PubMed
-
- Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
