

Lateral neck dissection surgeon volume and complications in head and neck endocrine malignancy
- PMID: 37727340
- PMCID: PMC10506124
- DOI: 10.21037/gs-22-385
Lateral neck dissection surgeon volume and complications in head and neck endocrine malignancy
Abstract
Background: Increased surgeon volume is associated with decreased complications for many surgeries, including thyroidectomy. We sought to use two national databases to assess for associations between surgeon volume and complications in patients undergoing lateral neck dissection for thyroid or parathyroid malignancy.
Methods: Lateral neck dissections for thyroid and parathyroid cancer from the Nationwide Inpatient Sample and State Inpatient Database were analyzed. The primary outcome was any inpatient complication common to thyroidectomy, parathyroidectomy, or lateral neck dissection. The principle independent variable was surgeon volume. Multivariable analysis was then performed on this retrospective cohort study.
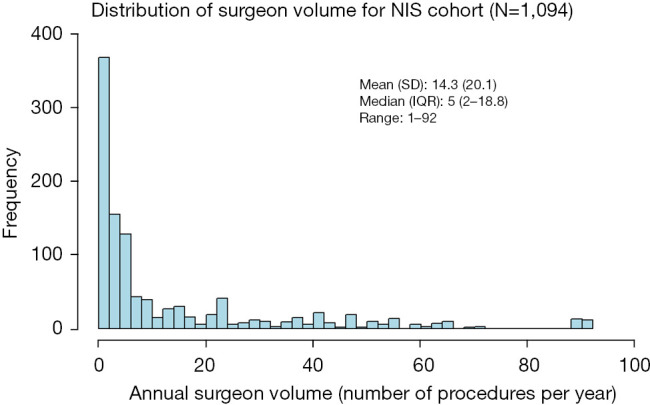
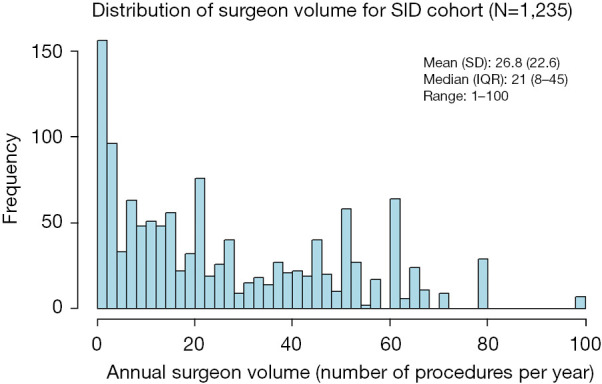
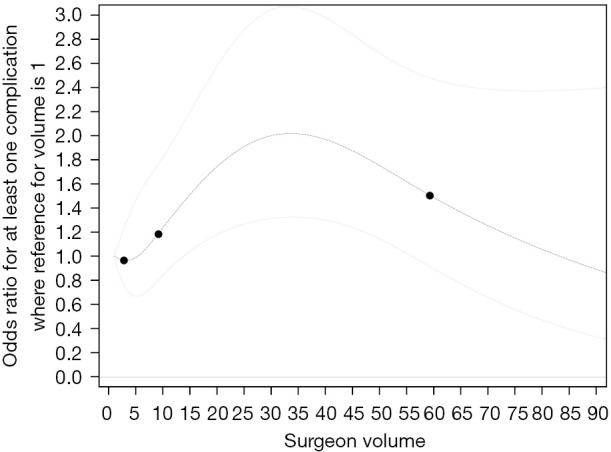
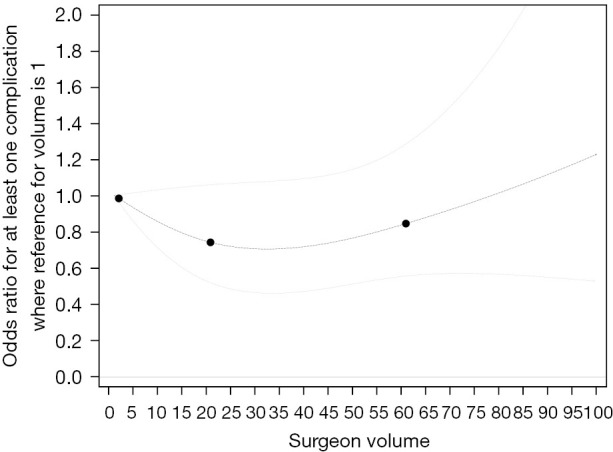
Results: The 1,094 Nationwide Inpatient Sample discharges had a 28% (305/1,094) complication rate. After adjustment, surgeons with volumes between 3-34 neck dissections/year demonstrated a surgeon volume-complication rate association [adjusted odds ratio: 1.03; 95% confidence interval (CI): 1.01-1.05]. The 1,235 State inpatient Database discharges had a 21% (258/1,235) overall complication rate, and no association between surgeon volume and complication rates (P=0.25).
Conclusions: This retrospective review of 2,329 discharges for patients undergoing lateral neck dissection for thyroid or parathyroidectomy demonstrated somewhat conflicting results. The Nationwide Inpatient Sample demonstrated increasing complication rates for increasing surgeon volume among intermediate volume surgeons, while the State Inpatient Database demonstrated no surgeon volume-complication association. Given these disparate results, and further limitations with these databases, conclusions regarding surgical volume and clinical decision making based on these data should be assessed cautiously.
Keywords: Neck dissection; parathyroid cancer; surgeon volume (SV); surgical outcomes; thyroid cancer.
2023 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://gs.amegroups.com/article/view/10.21037/gs-22-385/coif). TYC reports that she receives consulting fees from Cook Medical for lectures on implantable dopplers. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Surgeon Volume and Complications in Lateral Neck Dissection for Squamous Cell Carcinoma: A Multidatabase Analysis.Otolaryngol Head Neck Surg. 2021 Dec;165(6):838-844. doi: 10.1177/01945998211000438. Epub 2021 Mar 9. Otolaryngol Head Neck Surg. 2021. PMID: 33689518
-
Incidental parathyroidectomy in thyroidectomy and central neck dissection.Surgery. 2021 May;169(5):1145-1151. doi: 10.1016/j.surg.2020.11.023. Epub 2021 Jan 11. Surgery. 2021. PMID: 33446359
-
Optimal surgeon-volume threshold for neck dissections in the setting of primary thyroid malignancies.Surgery. 2022 Jan;171(1):172-176. doi: 10.1016/j.surg.2021.04.046. Epub 2021 Jul 12. Surgery. 2022. PMID: 34266647
-
Thyroid and parathyroid surgeon case volume influences patient outcomes: A systematic review.Surg Oncol. 2021 Sep;38:101550. doi: 10.1016/j.suronc.2021.101550. Epub 2021 Apr 6. Surg Oncol. 2021. PMID: 33915486
-
Endocrine Surgery: Management of Postoperative Complications Following Endocrine Surgery of the Neck.Surg Clin North Am. 2021 Oct;101(5):767-784. doi: 10.1016/j.suc.2021.05.019. Epub 2021 Aug 2. Surg Clin North Am. 2021. PMID: 34537142 Review.
Cited by
-
Treatment outcomes in patients with papillary thyroid cancer undergoing radiofrequency ablation of metastatic lymph nodes.Gland Surg. 2024 Oct 31;13(10):1752-1758. doi: 10.21037/gs-24-285. Epub 2024 Oct 26. Gland Surg. 2024. PMID: 39544984 Free PMC article.
-
An Analysis of Primary Hyperparathyroidism in Individuals Diagnosed with Multiple Endocrine Neoplasia Type 2.Diseases. 2025 Mar 27;13(4):98. doi: 10.3390/diseases13040098. Diseases. 2025. PMID: 40277809 Free PMC article. Review.
References
-
- Naso WB, Rhea AH, Poole A. Management and outcomes in a low-volume cerebral aneurysm practice. Neurosurgery 2001;48:91-9; discussion 99-100. - PubMed
-
- Wenner J, Zilling T, Bladström A, et al. The influence of surgical volume on hospital mortality and 5-year survival for carcinoma of the oesophagus and gastric cardia. Anticancer Res 2005;25:419-24. - PubMed
LinkOut - more resources
Full Text Sources